
Contraception and Family Planning — MCQs

On this page
A 25-year-old lady is undergoing manual vacuum aspiration for an unplanned conception. The maximum negative pressure generated during the procedure is: (DNB Pattern 2018)
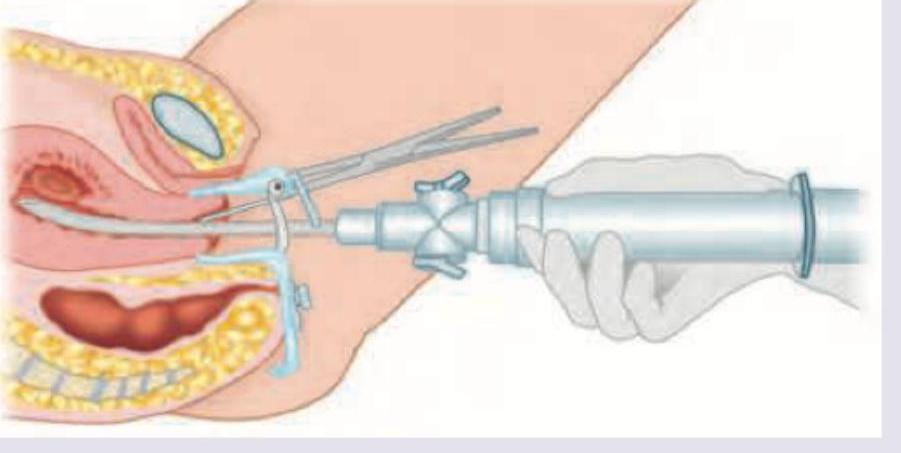
Aspiration with the instrument shown is termed menstrual regulation when performed within how many days of a missed period?

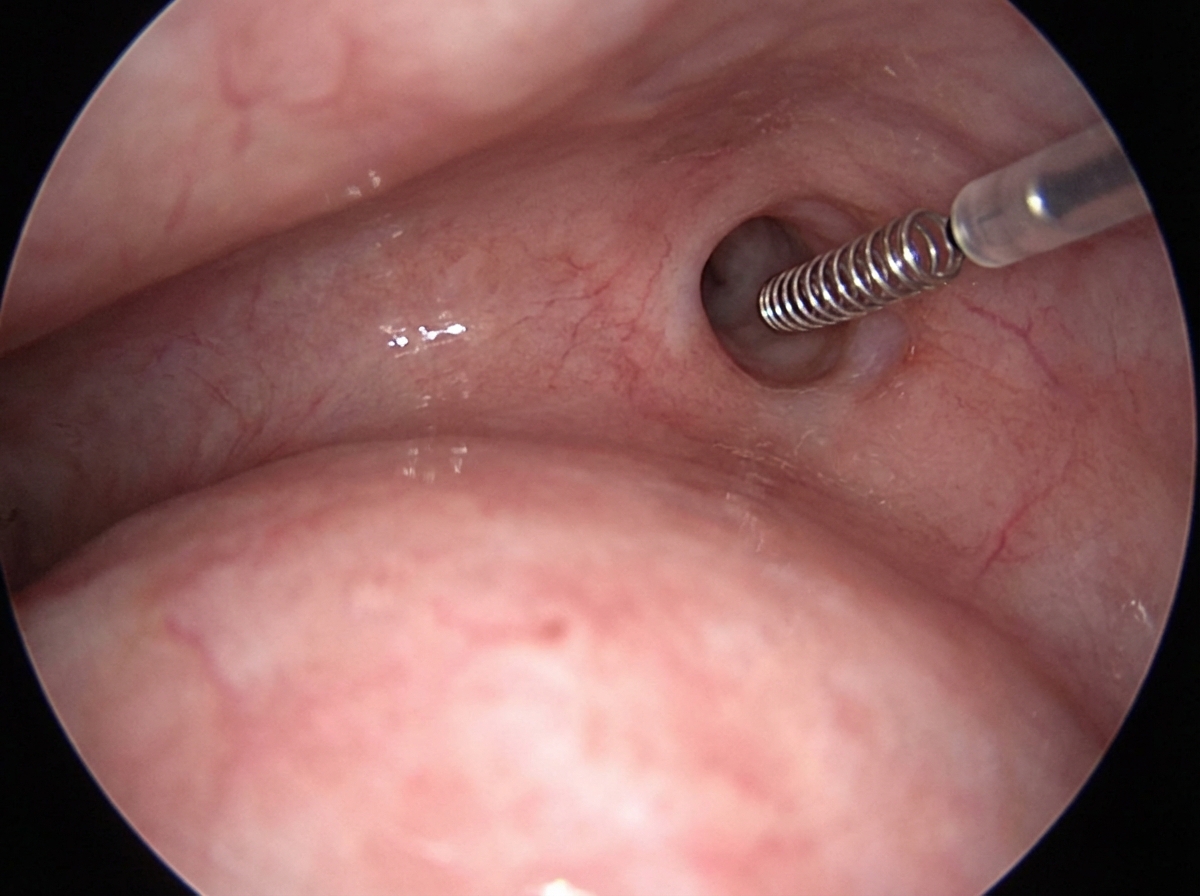
The sterilization method shown here is known as: (DNB Pattern 2018)
The most popular technique of tubal ligation is :
Which of the following statements regarding female sterilization is correct? 1. It can be done 24 - 48 hours following delivery. 2. Ideal time for interval ligation is luteal phase preceding menstruation. 3. It can be combined with medical termination of pregnancy. 4. It is a preventive measure against serous ovarian cancer. Select the correct answer using the code given below:
A 27-year-old recently married female comes to family planning clinic requesting for long term reversible contraception. Which one of the following is the best suited option for her ?
Which of the following are the absolute contraindications for the use of combined oral contraceptive pills ? 1. Severe hypertension 2. Pregnancy 3. Diabetes with retinopathy 4. Gall bladder disease Select the correct answer using the code given below :
Indication for removal of IUDs include which of the following ? 1. Perforation of uterus 2. Pregnancy with device in situ 3. One year after menopause 4. Persistent migraine Select the correct answer using the code given below :
How many times in a year does withdrawal bleeding occur in extended continuous regimens of combined oral contraceptive pills?
Which of the following are examples of LARC (Long Acting Reversible Contraceptives) ? 1. Copper-T 380A 2. Implants 3. LNG-IUS Select the correct answer using the code given below :
Practice by Chapter
Natural Family Planning Methods
Practice Questions
Barrier Methods
Practice Questions
Hormonal Contraceptives
Practice Questions
Intrauterine Devices
Practice Questions
Emergency Contraception
Practice Questions
Permanent Contraception Methods
Practice Questions
Contraception in Special Populations
Practice Questions
Contraceptive Counseling
Practice Questions
Side Effects and Complications of Contraceptives
Practice Questions
Future Contraceptive Technologies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app