
Contraception and Family Planning — MCQs

On this page
What is the following contraceptive method called?

Identify the contraceptive method shown below:

Identify the instrument shown in the image:

The X-ray pelvis AP shows presence of:

The following picture shows a contraceptive. All are correct about the device except:

The non-steroidal oral contraceptive Saheli (ormeloxifene) acts primarily by:

A patient has received the following birth control method. It is called:

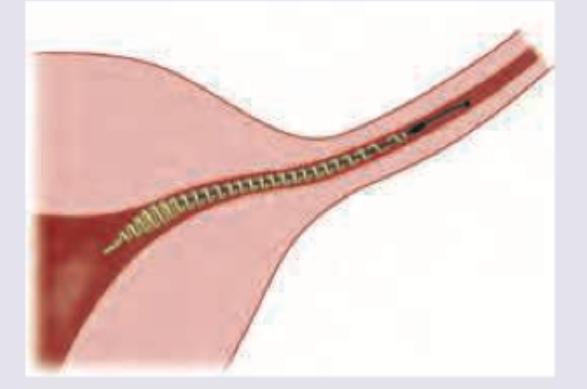
The contraception method shown below has an outer coil made of:
Identify the laparoscopic tubal sterilization shown below.

What is the method of contraception shown below?

Practice by Chapter
Natural Family Planning Methods
Practice Questions
Barrier Methods
Practice Questions
Hormonal Contraceptives
Practice Questions
Intrauterine Devices
Practice Questions
Emergency Contraception
Practice Questions
Permanent Contraception Methods
Practice Questions
Contraception in Special Populations
Practice Questions
Contraceptive Counseling
Practice Questions
Side Effects and Complications of Contraceptives
Practice Questions
Future Contraceptive Technologies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app