
Contraception and Family Planning — MCQs

On this page
OCPs are not protective for?
A 32-year-old woman presents with intermenstrual bleeding following the insertion of an intrauterine device (IUD). She reports no other complications. What is the most appropriate initial management step?
Identify the image given below:
Identify the image given below:
Identify the image given below:
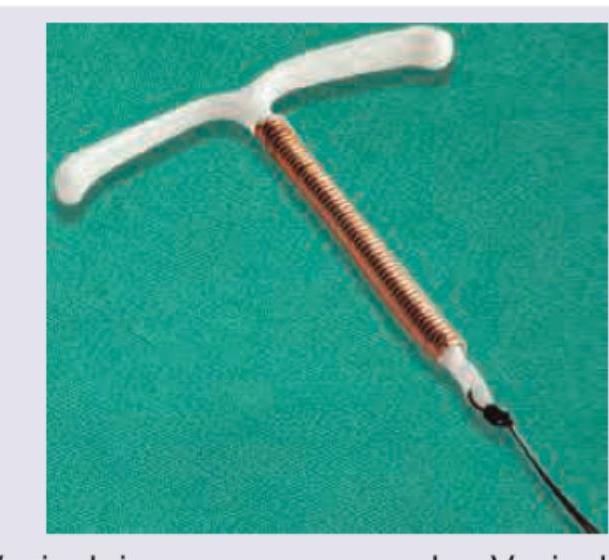
Which method of contraception is shown below?
Which of the following is true about the pill shown in the image?
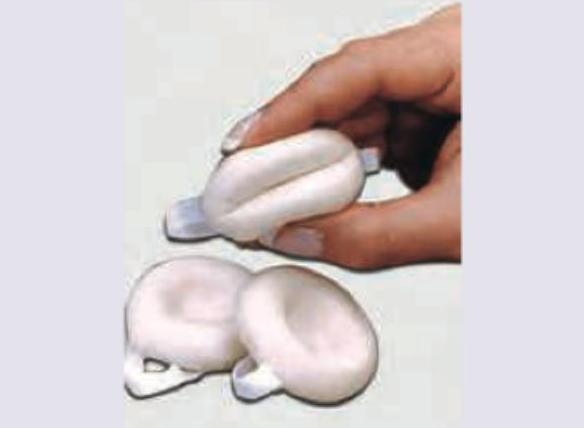
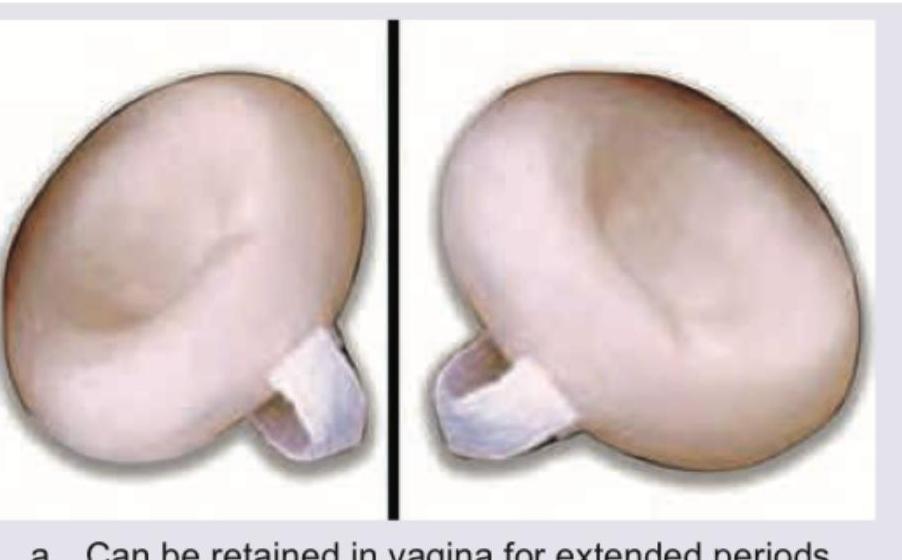
What is the most distinctive functional characteristic of the barrier method shown?
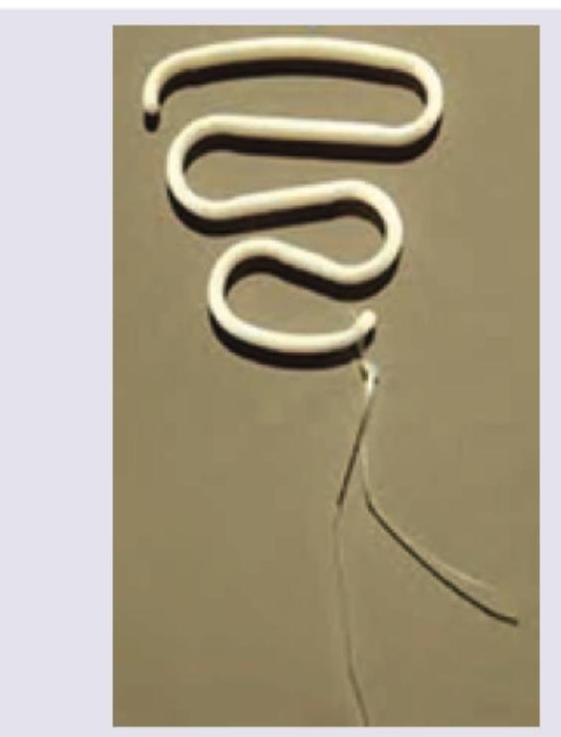
What is the contraceptive method shown in the image called?

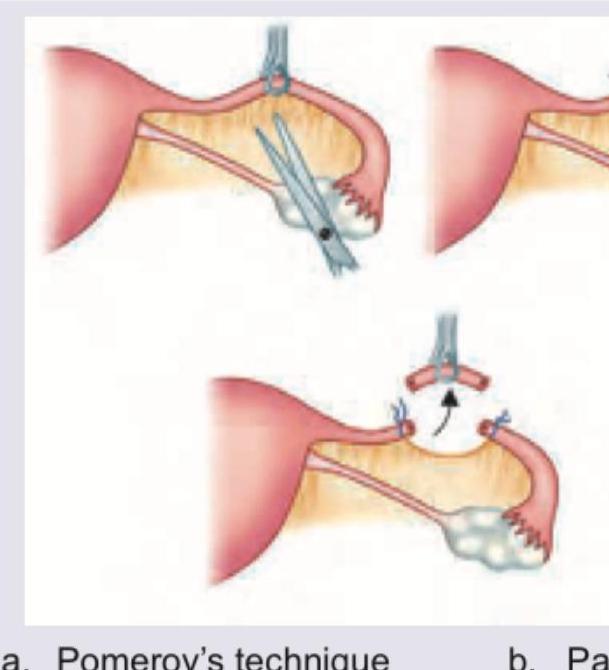
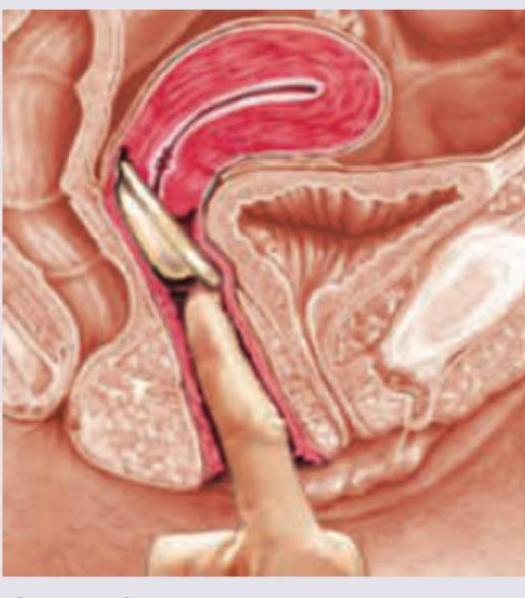
Which method of contraception usage is shown here?
Practice by Chapter
Natural Family Planning Methods
Practice Questions
Barrier Methods
Practice Questions
Hormonal Contraceptives
Practice Questions
Intrauterine Devices
Practice Questions
Emergency Contraception
Practice Questions
Permanent Contraception Methods
Practice Questions
Contraception in Special Populations
Practice Questions
Contraceptive Counseling
Practice Questions
Side Effects and Complications of Contraceptives
Practice Questions
Future Contraceptive Technologies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app