
Contraception and Family Planning — MCQs

On this page
Regarding the given mode of contraception, all statements are true EXCEPT?
Reversal of sterilization is best achieved by which method?
Oral contraceptive pills predispose to which of the following conditions?
Which of the following natural family planning methods is most effective?
What is the most commonly performed type of tubal ligation in current practice?
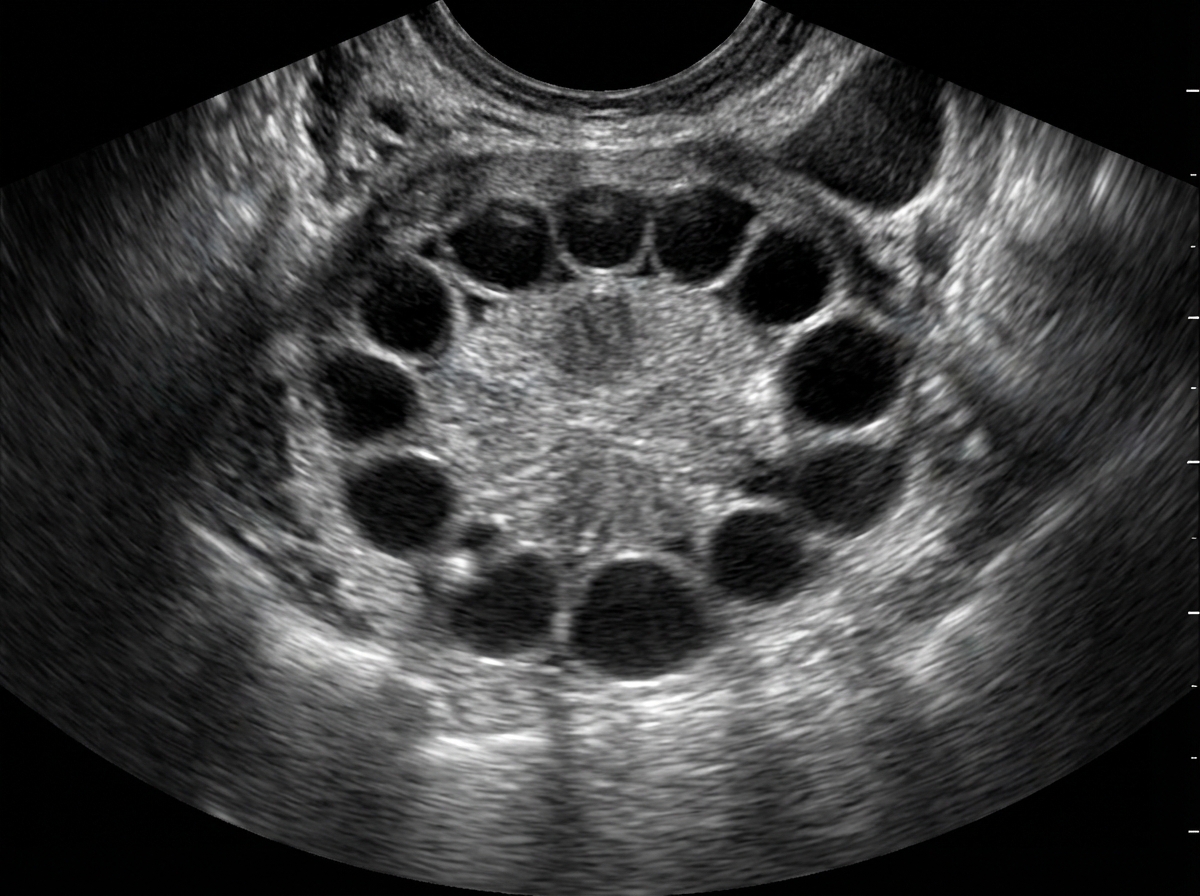
A 24-year-old woman presents with a diagnosis of PCOS, irregular and heavy menstrual cycles, and a desire for contraception and cycle control. She has no contraindications to estrogen. What is the ideal contraceptive in the given scenario?
What is the absolute contraindication for prescribing oral contraceptive pills in a woman of reproductive age group?
Which is the most likely complication of an IUD?
What is the primary mechanism of action of combined oral contraceptive pills?
Which one of the following statements regarding the female contraceptive "Today" is true?
Practice by Chapter
Natural Family Planning Methods
Practice Questions
Barrier Methods
Practice Questions
Hormonal Contraceptives
Practice Questions
Intrauterine Devices
Practice Questions
Emergency Contraception
Practice Questions
Permanent Contraception Methods
Practice Questions
Contraception in Special Populations
Practice Questions
Contraceptive Counseling
Practice Questions
Side Effects and Complications of Contraceptives
Practice Questions
Future Contraceptive Technologies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app