
Contraception and Family Planning — MCQs

On this page
A 32-year-old woman presents for contraception counseling. Which of the following is a contraindication to the use of combined oral contraceptive pills?
A woman had a LNG -IUCD inserted. She has been experiencing bleeding since the day of insertion, which is affecting her daily activities, and she demands removal. What is the appropriate management?
Which contraception is contraindicated in a woman with hypertension?
What is the permanent method used for sterilization in females?
Which of the following statements regarding the HPV vaccine is correct?
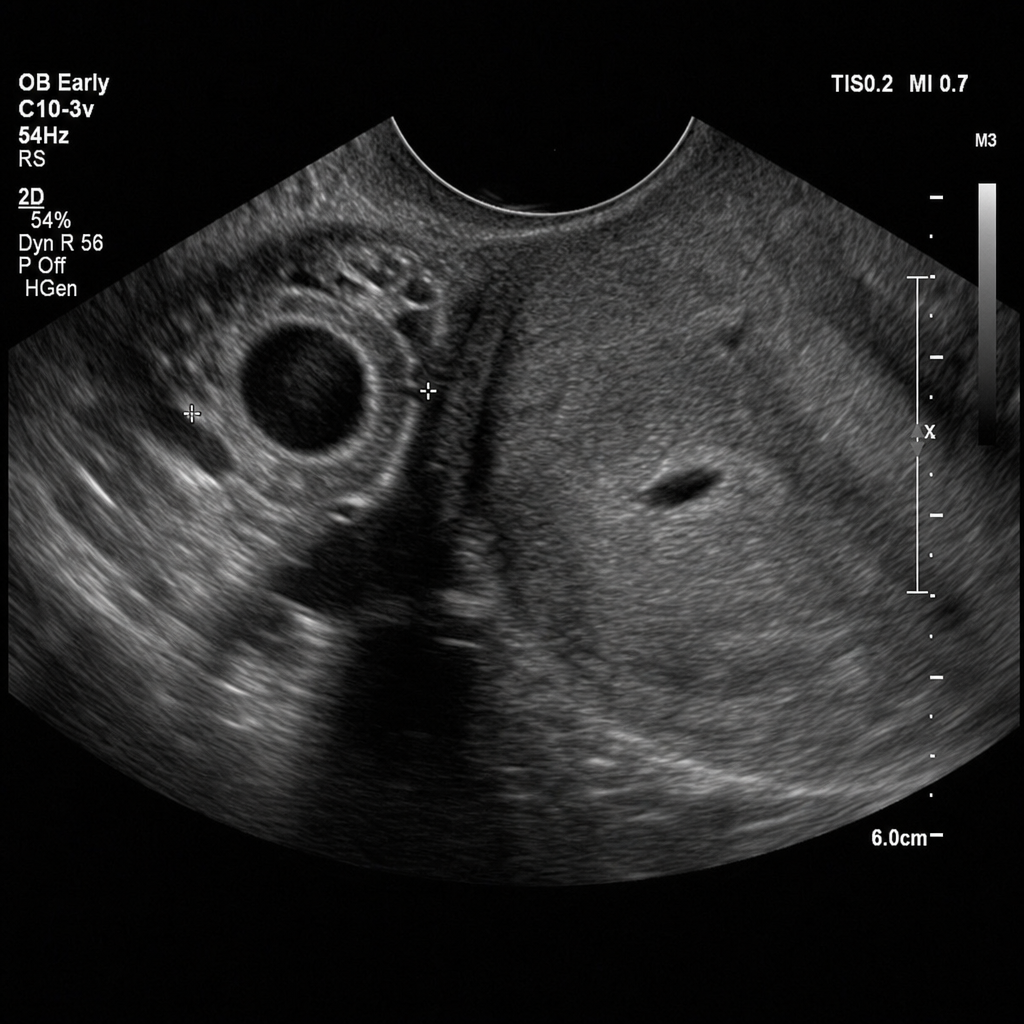
A 26-year-old woman with 6 weeks of amenorrhea presents to the emergency department with right iliac fossa pain and mild vaginal spotting. Her serum beta-hCG is 2400 mIU/mL. A transvaginal ultrasound is performed and is shown in Image 2, demonstrating an adnexal ring sign with an empty uterine cavity and no fetal cardiac activity on the right side. Her vital signs are: BP 112/74 mmHg, HR 88 bpm, she is hemodynamically stable. She has no contraindications to methotrexate (normal renal, hepatic, and hematologic function; no active pulmonary disease; no breastfeeding) and confirms she is able to comply with close outpatient follow-up. Which of the following is the most appropriate next step in management?
What is the ideal contraceptive for a couple who lives in different cities and meets only occasionally?
Which of the following is NOT an ideal candidate for insertion of an Intrauterine Contraceptive Device (IUCD)?
IUCD must not be used in a woman with which of the following conditions?
What is the most common side effect of IUD insertion?
Practice by Chapter
Natural Family Planning Methods
Practice Questions
Barrier Methods
Practice Questions
Hormonal Contraceptives
Practice Questions
Intrauterine Devices
Practice Questions
Emergency Contraception
Practice Questions
Permanent Contraception Methods
Practice Questions
Contraception in Special Populations
Practice Questions
Contraceptive Counseling
Practice Questions
Side Effects and Complications of Contraceptives
Practice Questions
Future Contraceptive Technologies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app