
Syphilis — MCQs

A patient presents with suspected primary syphilis. Which sequence of tests provides the most cost-effective screening approach?
Which spirochete is the causative agent of syphilis?
A man who has a penile chancre appears in a hospital's emergency service. The VDRL test is negative. The most appropriate course of action for the physician in charge would be to
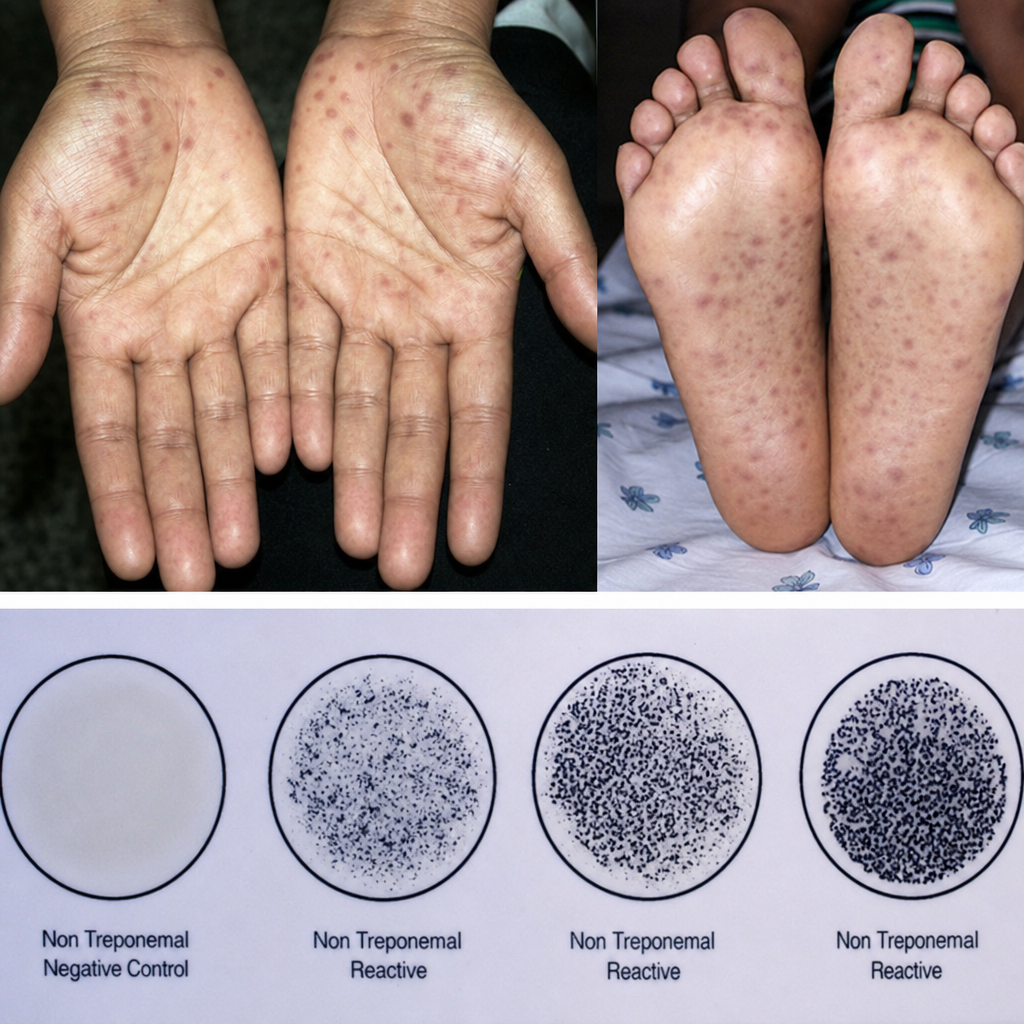
A 30-year-old pregnant female presented to the obstetrics OPD for the first time in the third trimester, at 36 weeks of gestation. She complained of fever, swollen lymph nodes, sore throat, and a characteristic rash on the palms as well as the soles of the feet. A serological screening test conducted in the given plate was positive for syphilis. Which of the following abnormalities can most likely be found in the child?
Symptoms of secondary syphilis are all except:
A young female with asymptomatic macules and papules over trunk and reddish patch over palate with a flat, moist lesion on vulva. Patient has generalized lymphadenopathy. What is the line of management?
A 40-year-old man with a history of untreated syphilis presents with ataxia, diminished deep tendon reflexes, and impaired vibratory and position sense. He was recently diagnosed with HIV (CD4 count 450/μL). VDRL is 1:8, and TPHA is positive. CSF shows pleocytosis, elevated protein, and positive VDRL. Which form of neurosyphilis is most likely?
Which part of the aorta is most commonly involved in syphilitic aneurysms?
Jarish-Herxheimer reaction is seen in early cases of what?
Painless ulcer along with painless lymphadenopathy is characteristic of which STD:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app