
Sleep-Related Movement Disorders — MCQs

A 50-year-old woman with schizophrenia who has been taking an antipsychotic drug for the past three years has begun to exhibit involuntary chewing and lip-smacking movements. Which is the most likely possibility?
Which condition is associated with periodic discharges on EEG at 4-second intervals?
A 32-year-old patient with Restless leg syndrome comes to the OPD. What is the most appropriate first line treatment?
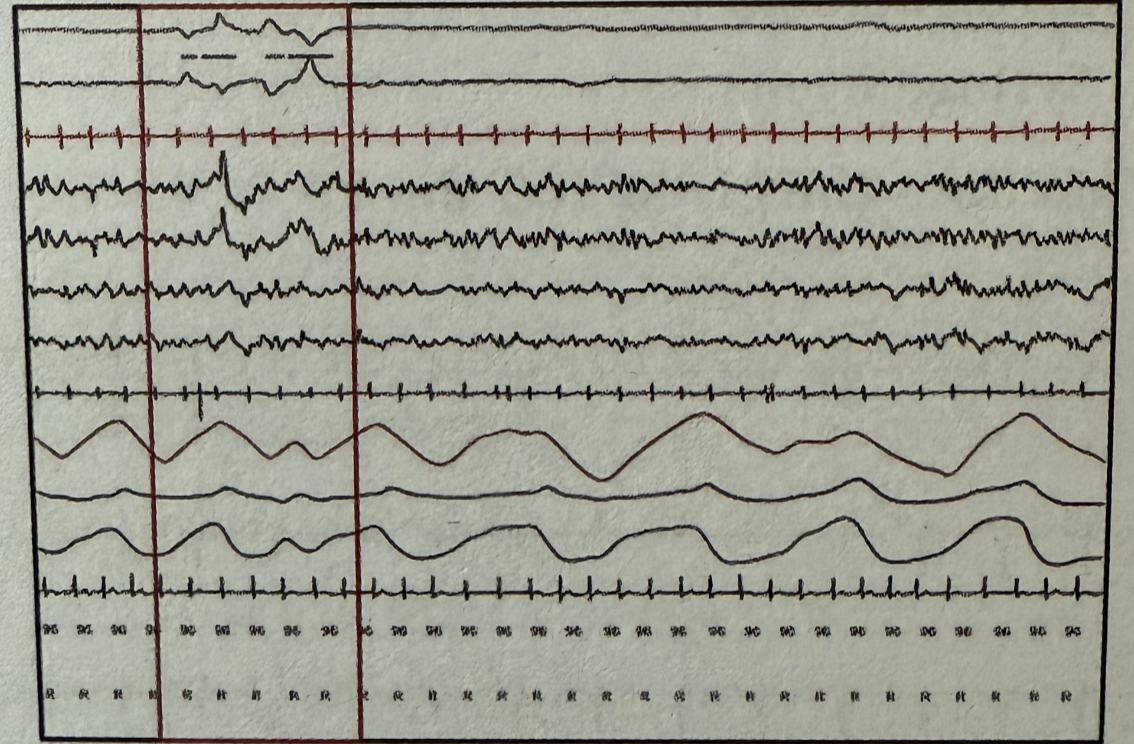
During polysomnography, which stage of sleep is represented by the marked areas when observing the following wave patterns? EOG (Electrooculography) EEG (Electroencephalography) EMG (Electromyography)
A 60-year-old man with Parkinson’s disease presents with visual hallucinations and cognitive decline over the past year. He is on levodopa. What is the most likely diagnosis?
A 55-year-old woman presents with widespread pain, fatigue, and sleep disturbances. Physical examination reveals multiple tender points. What is the most likely diagnosis?
In narcolepsy, the polysomnographic recording typically shows which of the following patterns?
Muller's manoeuvre is used to
A 55-year-old man presents with a tremor that occurs when his hands are at rest. He has a slow, shuffling gait and difficulty initiating movement. His symptoms improve with levodopa. What is the most likely diagnosis?
All of the following decrease in iron deficiency anemia except:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app