
Sleep Medicine — MCQs

On this page
Non-erosive arthritis is characteristic of which condition?
Sleep apnea is defined as a temporary pause in breathing during sleep lasting at least:
An obese, diabetic patient with hypertension, who is also a smoker and currently on anti-hypertensive and oral hypoglycemic drugs, presents with complaints of apnea during sleep. Polysomnography reveals 5 apneic episodes and 1 hypopneic episode per hour. What is the best next line of management?
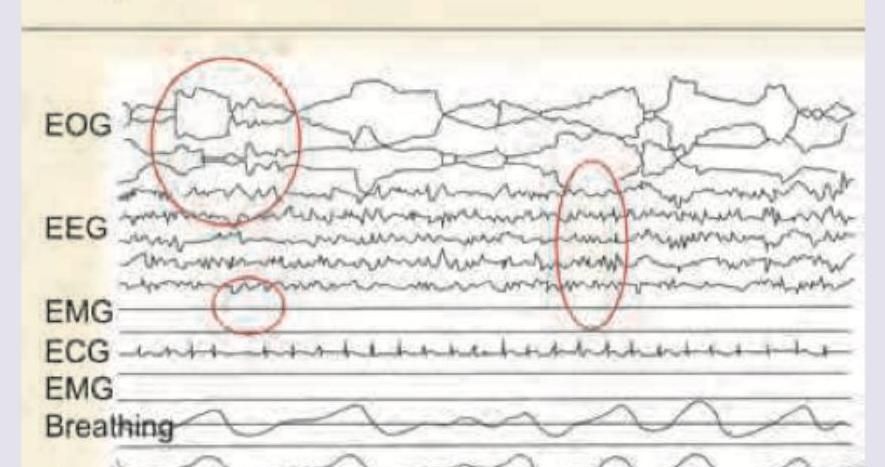
Identify the sleep stage in the following Polysomnograph.
A 40-year-old man presents with daytime sleepiness and impaired concentration and memory. On examination his BMI is 41 kg/m2, BP is 160/100 mm Hg. His awake ABG analysis is given: PaO2=66 mm Hg, PaCO2=50 mm Hg, HCO3=28 mEq/L. What is the most likely diagnosis?
A 45-year-old obese man presents to his primary care provider for an annual physical. The patient states that he has noticed increased sleepiness during the day at work over the past 6 months in addition to difficulty concentrating and worsening memory. He denies recent weight loss, and is not sure if he snores because he sleeps by himself. His past medical history is significant for hypertension and type II diabetes. Vital signs are T 98.6 F, HR 75 bpm, BP 140/90 mm Hg, RR 18/min. Physical exam reveals a 350 pound man. Jugular venous distension is difficult to evaluate due to excess tissue in the neck. There is no peripheral edema. Lung exam is normal. Routine CBC shows WBC count of 5000 cells/ml, platelet count of 350,000/mcL, hemoglobin of 18 gm/dL, and hematocrit of 54%. What is the most likely cause of his abnormal lab results?
The sleep apnea syndrome is defined as -
What is the minimum diagnostic threshold for obstructive sleep apnoea according to current guidelines?
Muller's manoeuvre is used to
A 32-year-old patient with Restless leg syndrome comes to the OPD. What is the most appropriate first line treatment?
Practice by Chapter
Normal Sleep Physiology
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Insomnia
Practice Questions
Hypersomnias
Practice Questions
Circadian Rhythm Disorders
Practice Questions
Parasomnias
Practice Questions
Sleep-Related Movement Disorders
Practice Questions
Sleep in Medical Disorders
Practice Questions
Sleep in Psychiatric Disorders
Practice Questions
Sleep Diagnostics
Practice Questions
Pharmacologic Management of Sleep Disorders
Practice Questions
Non-pharmacologic Sleep Interventions
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app