
Cross-Cultural Medicine — MCQs

Which of the following is not a two-way communication?
In implementation of a health programme, best thing to do is -
The MOST effective strategy to change health behaviors and attitudes of people is
The BEINGS Model of disease causation does not include which of the following factors?
Population norm for Health Assistants in tribal areas:
Comprehension difficulty in the receiver is a _________ type of barrier of communication
Which of the following is a feature of mass media education?
A mother delivers in a rural area under the guidance of a skilled care attendant. Which of the following statements is incorrect regarding the care provided by the skilled care attendant at birth?
What is the primary health concern addressed by the Rashtriya Bal Swasthya Karyakram (RBSK)?
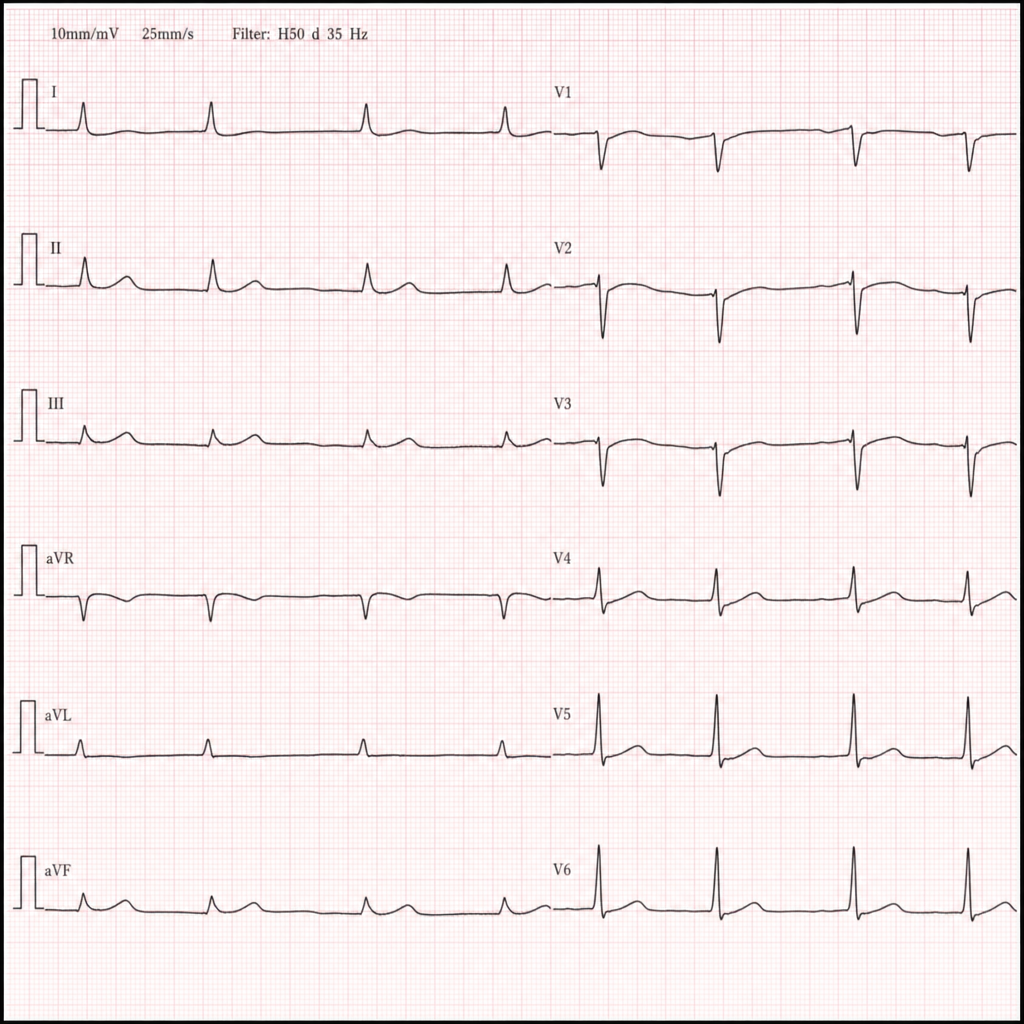
A homeless man is brought to the emergency department in January after being found unresponsive in a park. He is bradycardic and minimally responsive. A 12-lead ECG is obtained (Image 1). Which of the following is the most likely life-threatening arrhythmia if this patient's core temperature is not corrected?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app