
Oncology — MCQs

On this page
Which of the following is NOT included in the management of febrile neutropenic patients receiving anti-cancer therapy?
Which is the most common metastatic disease causing Superior Vena Cava (SVC) syndrome?
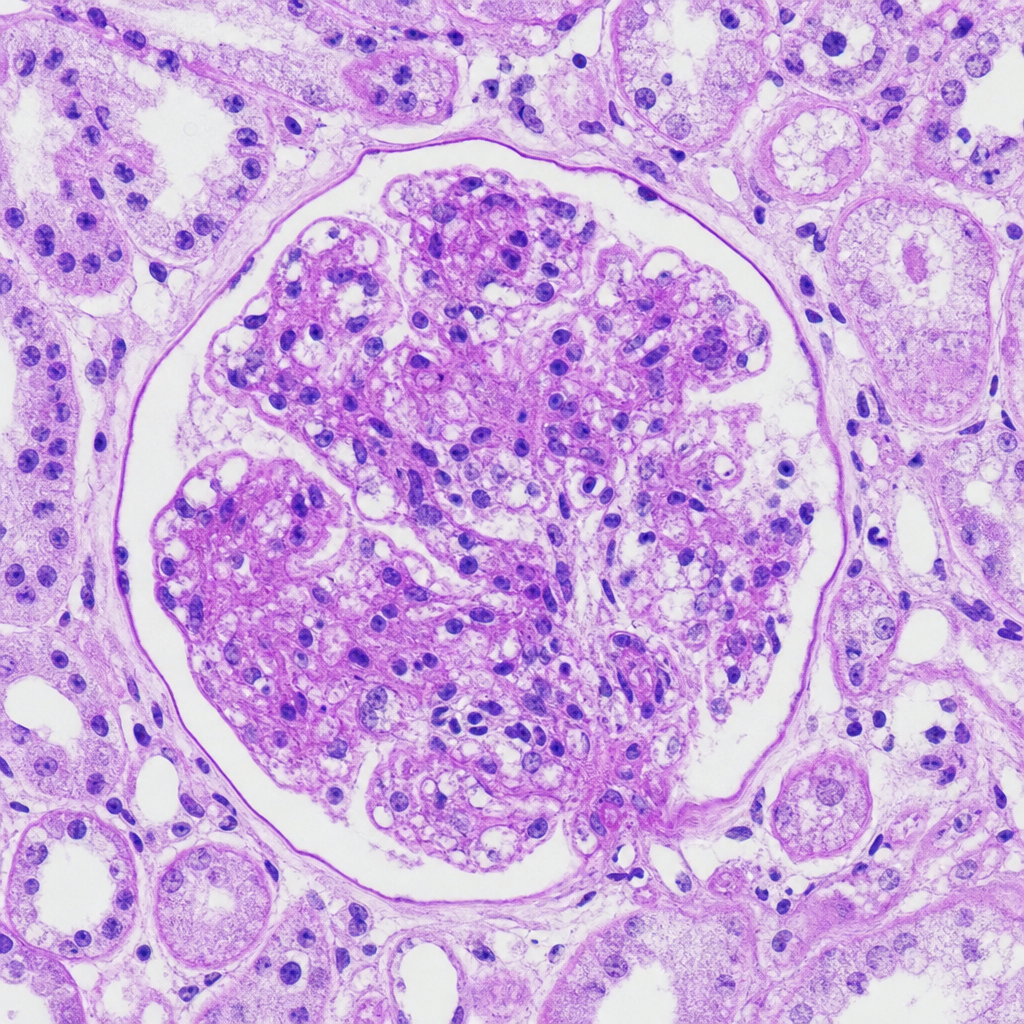
A 14-year-old girl presents with a rash, abdominal pain, arthralgias, nausea, vomiting, and bloody stools. Physical examination reveals a palpable purpuric rash on her buttocks and lower legs, a tender abdomen, and no active joint inflammation. Urinalysis shows RBCs and RBC casts, and her renal function deteriorates rapidly. A renal biopsy is performed showing mesangial and endocapillary hypercellularity without extracapillary crescent formation in the sampled glomerulus. Considering the clinical presentation and biopsy findings, what is the most likely pattern on renal biopsy for this patient with glomerulonephritis (GN)?
Which parameter best predicts the return of renal function in a patient with tumor lysis syndrome?
Which of the following statements regarding the Philadelphia chromosome is NOT true?
A 50-year-old woman presents with pain and swelling in her proximal interphalangeal joints, wrists, and knees, accompanied by morning stiffness. She has a history of hysterectomy 10 years ago. Physical examination reveals swelling and synovial thickening of the proximal interphalangeal (PIP) joints. Her laboratory findings include: Hemoglobin 10.3 g/dL, MCV 80 fL, serum iron 28 mg/dL, iron-binding capacity 200 mg/dL, and saturation 14%. What is the most likely explanation for this woman's anemia?
A 69-year-old man with a 60 pack-year smoking history presents with dizziness and visual disturbances. Physical examination reveals a purplish discoloration of his face, arms, and neck; retinal vein engorgement; and visible distention of his neck veins. His complete blood count reveals a normocytic anemia. The pathophysiology of this patient’s clinical presentation most likely involves which of the following?
Which of the following is NOT recommended for the management of Tumour lysis syndrome?
What is the most common cause of carcinomatous meningitis?
Which of the following is NOT a paraneoplastic manifestation of bronchogenic carcinoma?
Practice by Chapter
Cancer Biology and Carcinogenesis
Practice Questions
Principles of Cancer Diagnosis and Staging
Practice Questions
Solid Tumor Management
Practice Questions
Hematological Malignancies
Practice Questions
Cancer Emergencies
Practice Questions
Principles of Chemotherapy, Immunotherapy and Targeted Therapy
Practice Questions
Radiation Oncology Basics
Practice Questions
Palliative Care in Oncology
Practice Questions
Cancer Screening and Prevention
Practice Questions
Paraneoplastic Syndromes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app