
Hypertension in Kidney Disease — MCQs

A hypertensive diabetic patient with microalbuminuria should receive:
A CKD patient develops serum K+ 7.2 mEq/L without ECG changes. Best initial management?
What is the physiological response of the kidney during shock?
Which of the following is not an absolute indication for hemodialysis?
Assertion: ACE inhibitors are contraindicated in bilateral renal artery stenosis. Reason: They cause acute kidney injury by reducing efferent arteriolar tone.
"Tracking" of blood pressure means:
Which of the following antihypertensive drugs is avoided in patients with high serum uric acid levels?
A 40-year-old man with a known case of hypertension presented with multiple episodes of hematuria and loin pain. His elder brother passed away due to a stroke at the age of 40. What is the probable diagnosis based on the clinical presentation?
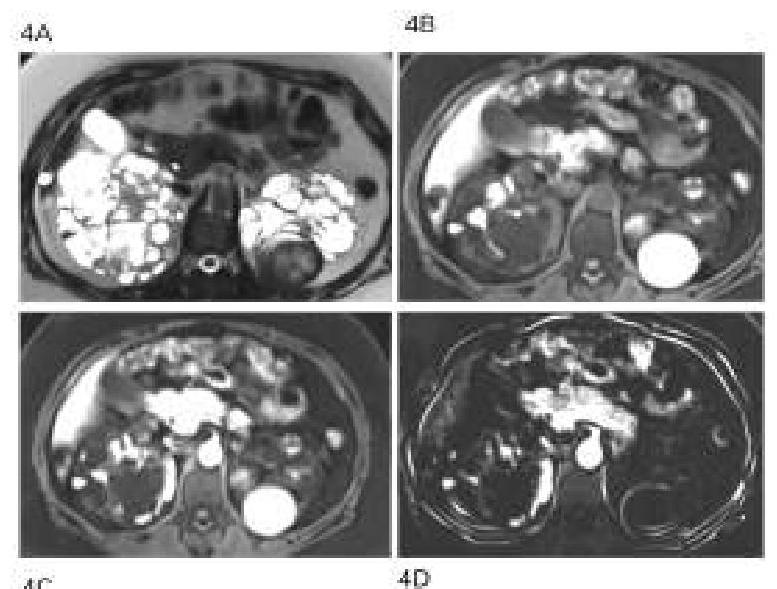
All the following are feature of polycystic disease of kidneys except:-
What is the primary effect of beta blockers in the management of thyroid storm?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app