
Anemia Evaluation and Management — MCQs

Which of the following is a feature of Vit B12 deficiency anemia?
Which parameter is primarily used to diagnose macrocytosis in a complete blood count (CBC)?
Earliest manifestation of megaloblastic anemia is
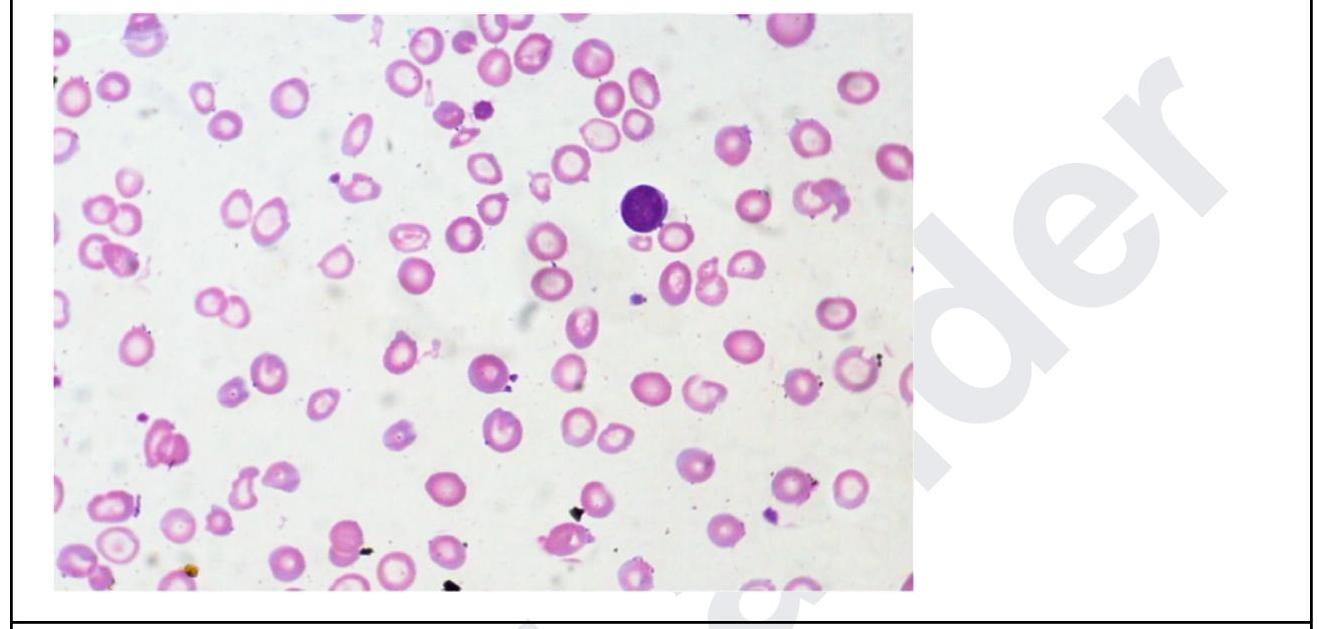
A 35 year old woman presents with fatigue. Investigations revealed the following: Hb, 5 g/dL; MCH, 24; low MCV; leukocytes, 11,000/ uL, and platelets, 5 lakhs. The peripheral smear is shown below. What is the diagnosis? Normal values: - Mean cell volume (MCV); 90 ± 8 fL - Mean cell Hb(MCH); 30 ± 3 pg
Anemia with reticulocytosis is seen in -
A patient has MCV <80, MCH <23. Which type of anaemia shall be classified?
What is a known complication of Parvovirus B19 infection?
Which of the following is not likely to be seen in a patient with Paroxysmal Nocturnal Hemoglobinuria (PNH)?
Bleeding crisis in acute idiopathic thrombo-cytopenic purpura is managed by all except -
A 40-year-old presents with cirrhosis and low ferritin. What is the next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app