
Gastroenterology — MCQs

On this page
What is the primary clinical application of the Rockall score?
Which of the following statements about alcoholic hepatitis is false?
Which of the following is not a characteristic of Zieve syndrome?
What is a potential risk factor for ulcerative colitis?
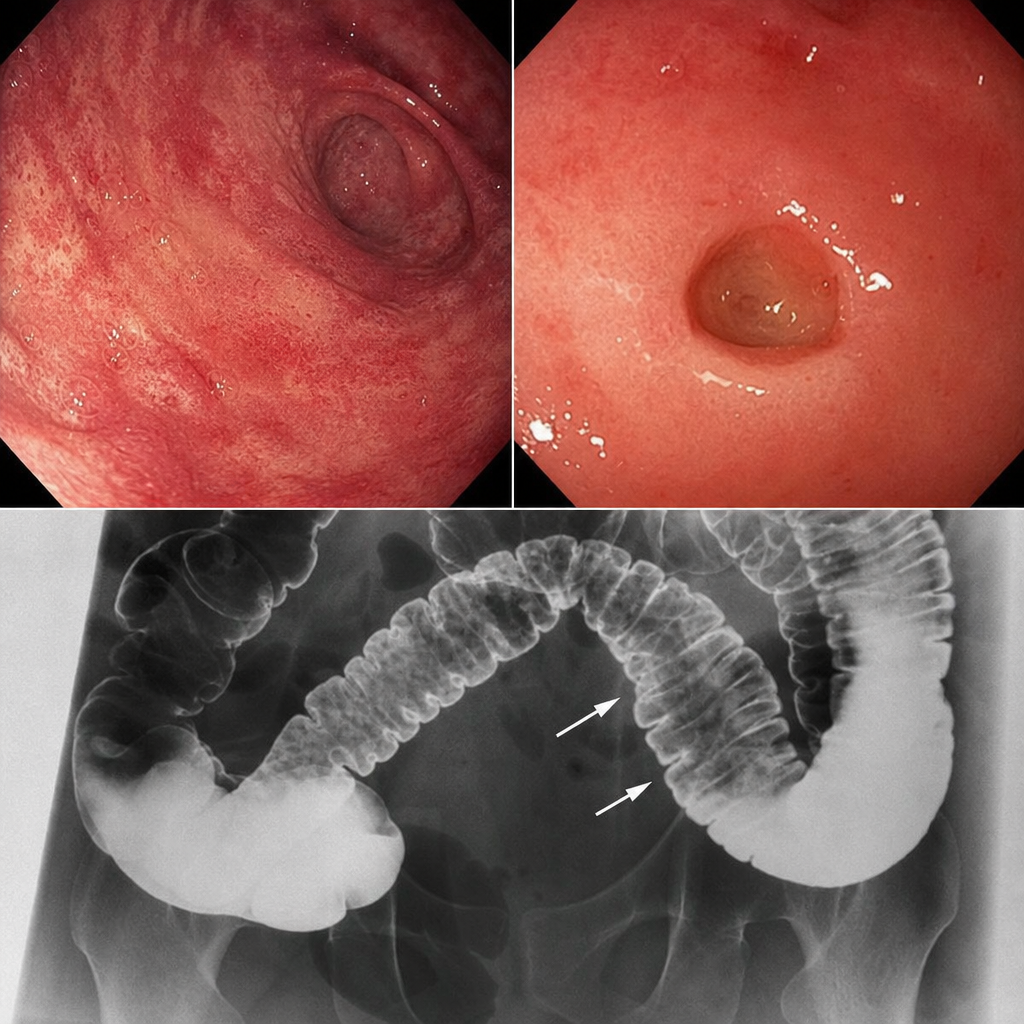
A patient presents with skin involvement and collar stud ulceration in the intestine observed on radiography. What is the most likely diagnosis?
In which non-neoplastic condition is CEA commonly elevated?
In which portion of the esophagus do esophageal varices primarily occur?
Wireless capsule endoscopy is done to visualize which of the following condition?
Genitourinary complication of ulcerative colitis
A 40-year-old male with gastroesophageal reflux disease (GERD) is found to have Barrett's esophagus with low-grade dysplasia on endoscopy. What is the most appropriate initial pharmacological treatment for this condition?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app