
Gastroenterology — MCQs

On this page
What is the most common cause of pyogenic liver abscess?
Investigation of choice for a 74-year-old male patient with scanty bleeding per rectum and irregular bowel habits.
Which of the following statements about blind loop syndrome is false?
Which vitamin is not deficient in celiac disease?
Which of the following is not a valid test for investigating fat malabsorption?
A patient comes with abdominal pain, jaundice, and portal hypertension. Anastomosis between which of the following veins is seen?
A 30-year-old male is found to be positive for HBsAg and HBeAg and is diagnosed with chronic hepatitis B. The patient's viral load is 2 × 10^5 IU/mL and ALT is elevated (2× upper limit of normal). What is the appropriate management in this patient?
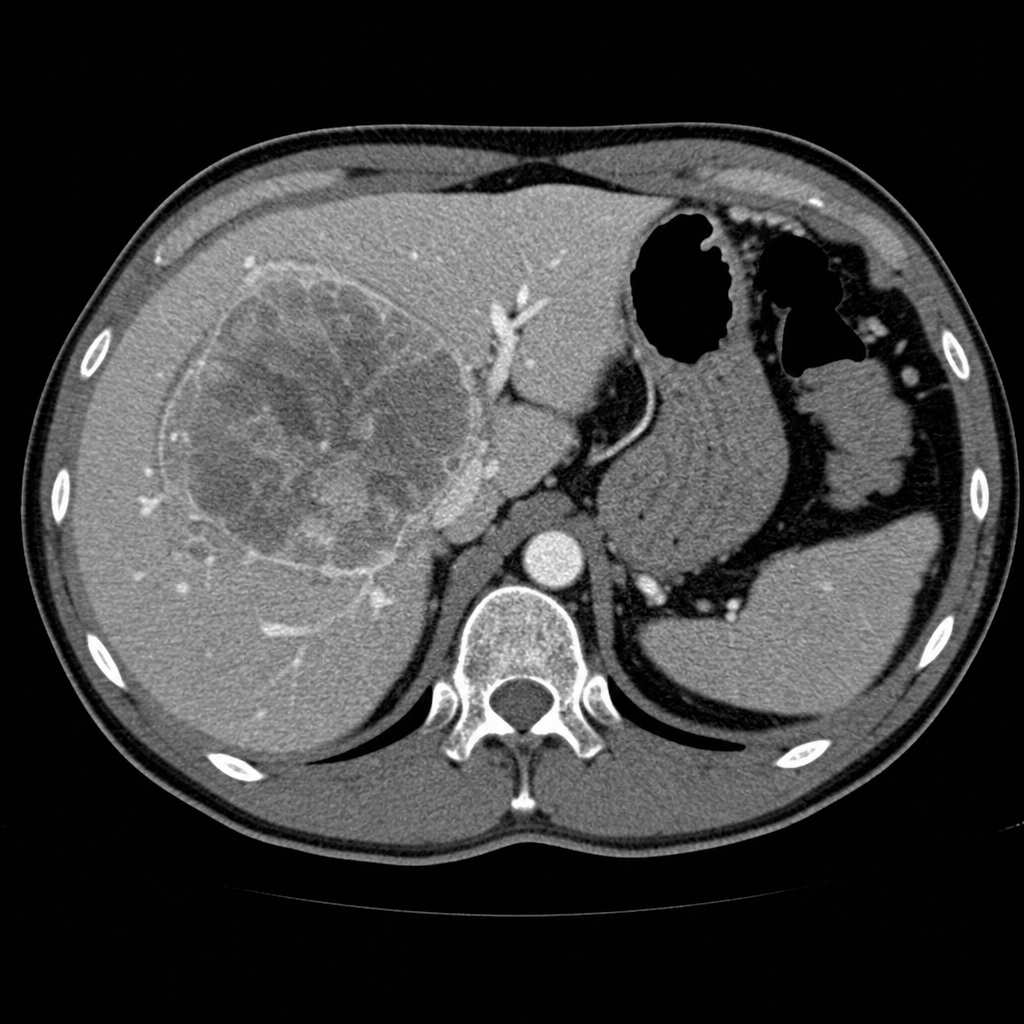
A patient with a history of alcohol dependence syndrome presents with sudden and unintentional weight loss. Laboratory results show an alpha-fetoprotein (AFP) level of 600 ng/mL, AST 180 U/L, ALT 90 U/L, and normal bilirubin levels. Imaging reveals underlying cirrhosis and a hepatic mass demonstrating arterial phase hyperenhancement and washout appearance in the portal venous phase on multiphasic CT. What is the most likely diagnosis?
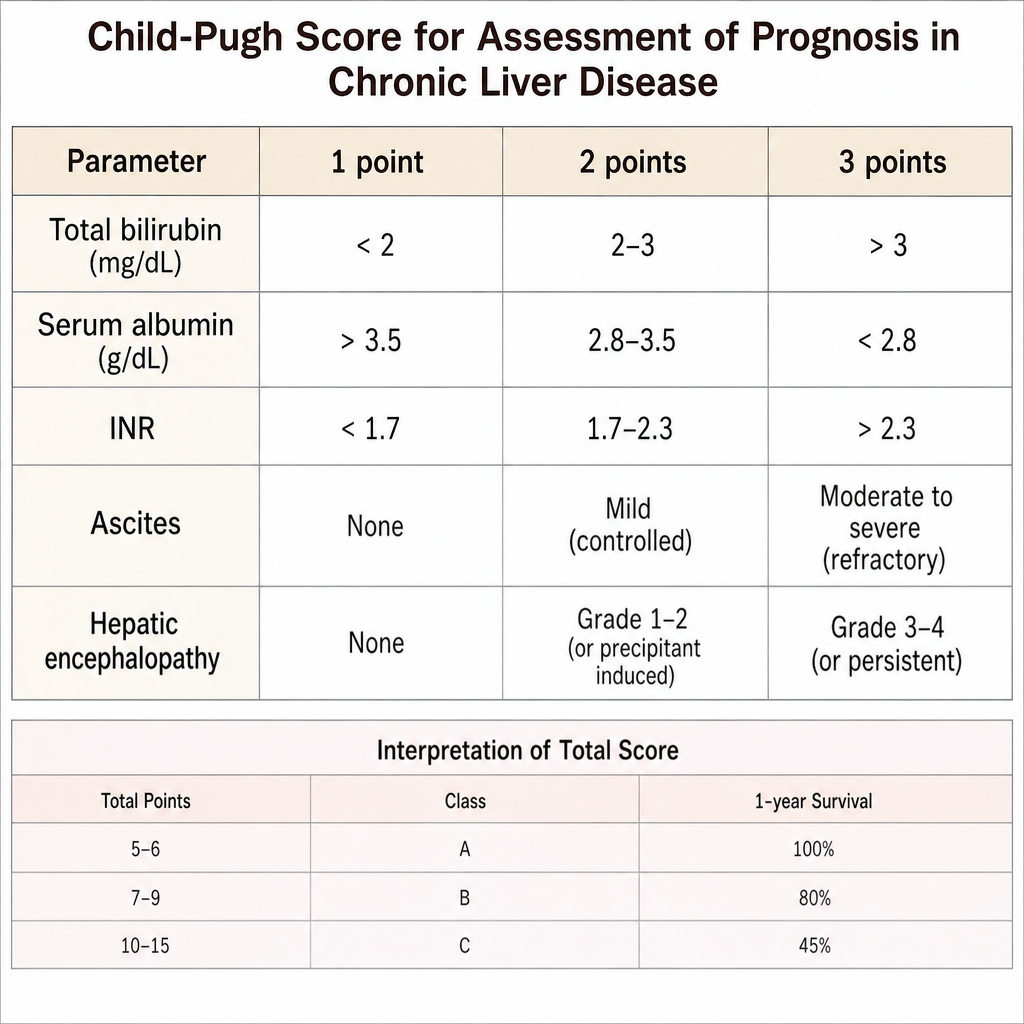
Which of the following scores uses bilirubin, albumin, INR, ascites, and encephalopathy to classify cirrhosis into classes A, B, and C?
Which of the following laboratory values is NOT a component of the MELD score?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app