
Gastroenterology — MCQs

On this page
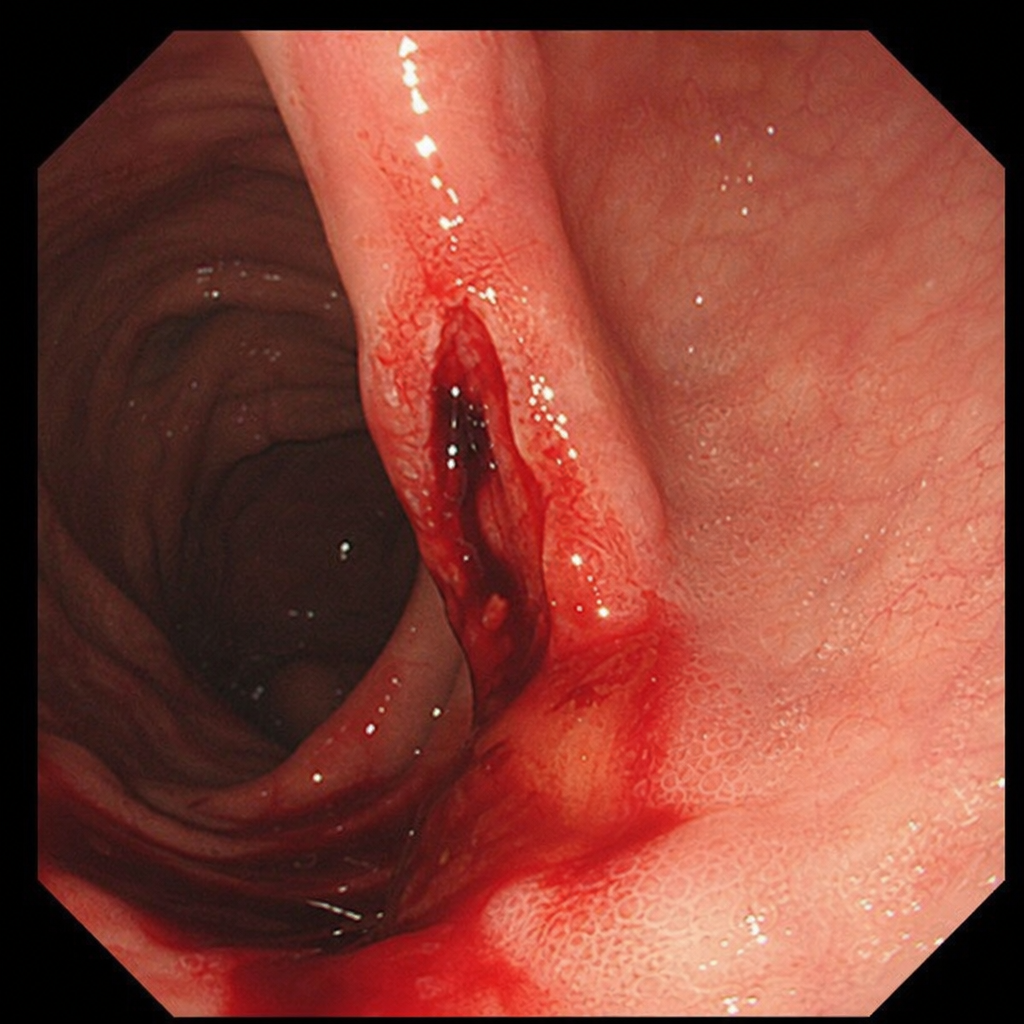
A 28-year-old pregnant female complains of hematemesis after an episode of vomiting. An upper GI endoscopy reveals a specific appearance. What is the most common site for this condition?
Which drug is used in the treatment of steroid-resistant ulcerative colitis?
Anti-T.T.G. antibodies are seen in which condition?
Which of the following factors predispose to hepatic encephalopathy?
A 40-year-old woman presents with severe abdominal pain localized to the right upper quadrant. A urine sample is taken for rapid dipstick reagent strip analysis. A positive result for which of the following substances would most strongly suggest gallstone disease as a possible cause of her abdominal pain?
Which grain can be used safely in Celiac sprue?
A person has a history of steatorrhea of long duration. D-xylose testing was performed. A 5-hour urine sample showed <4.5 g excretion after a 25g D-xylose load. What is/are the probable diagnosis?
In hepatic encephalopathy, what type of EEG activity is typically shown?
A patient presents with a history of diarrhea for several years and recent onset of pruritus and elevated alkaline phosphatase. Laboratory tests show normal SGOT/PT, and ultrasound reveals no gallstones or biliary tract abnormalities. What is the most likely diagnosis?
What is the treatment of choice for a patient with severe alcoholic hepatitis and a high discriminant function score?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app