
Gastroenterology — MCQs

On this page
A 45-year-old female presents with a long-standing history of heartburn and regurgitation. Endoscopy reveals Barrett's esophagus. What is the primary concern for this patient?
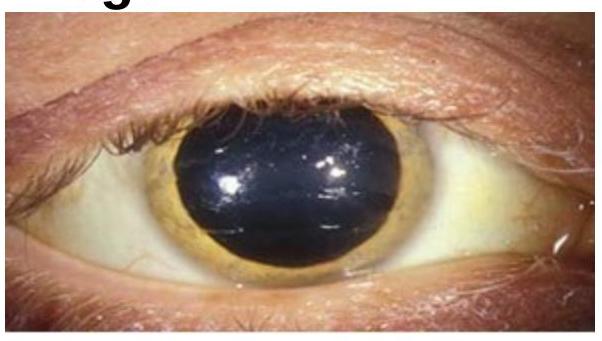
A 40-year-old man presents with liver disease and neurological symptoms. His serum ceruloplasmin levels are low. Which condition is most likely?
A 30-year-old female presents with progressive difficulty swallowing and a sensation of a lump in her throat. A barium swallow shows a filling defect in the esophagus. What is the most likely diagnosis?
Which test is most useful in differentiating between Irritable Bowel Syndrome (IBS) and organic gastrointestinal diseases?
Which of the following scores uses bilirubin, albumin, INR, ascites, and encephalopathy to classify cirrhosis severity?
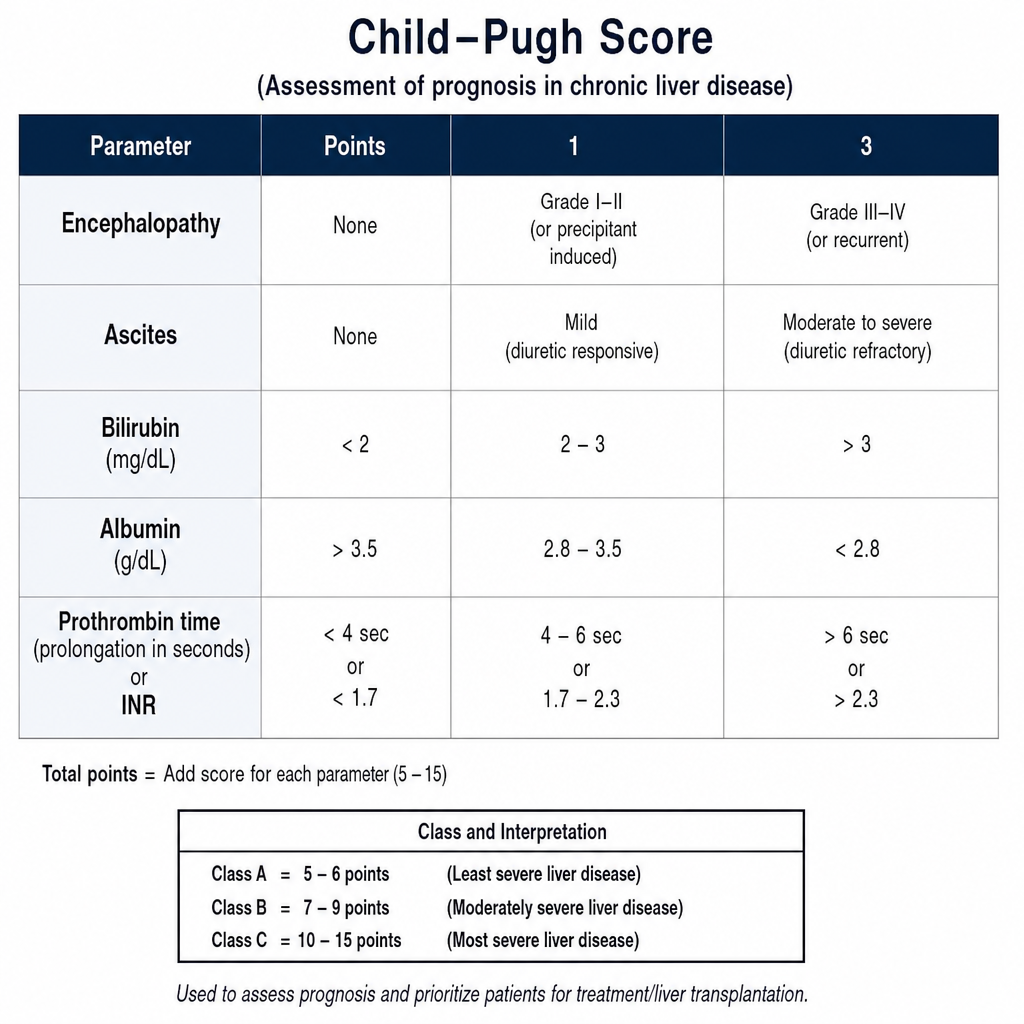
Which of the following laboratory values is NOT included in the MELD score?
Which laboratory test is most appropriate as an initial investigation for the underlying disorder?
Which enzyme is most specific for pancreatic pathology in the evaluation of chronic pancreatitis?
In men, what quantity of ethyl alcohol consumed daily for more than 10 years increases the relative risk of developing alcoholic liver disease?
Which of the following is MOST characteristic of gastric ulcers compared to duodenal ulcers?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app