
Gastroenterology — MCQs

On this page
What is the most common complication of acute pancreatitis?
According to Child-Pugh criteria, what does the presence of hepatic encephalopathy, a bilirubin level of 2.5 mg/dL, an albumin level of 3 gm/dL, and controlled ascites indicate?
A 55-year-old male patient presenting with gastritis symptoms was diagnosed with a gastric ulcer three years ago and underwent partial gastrectomy. He is currently on high-dose omeprazole. A follow-up endoscopy reveals two ulcerative lesions in the gastric mucosa. What is the next step in management?
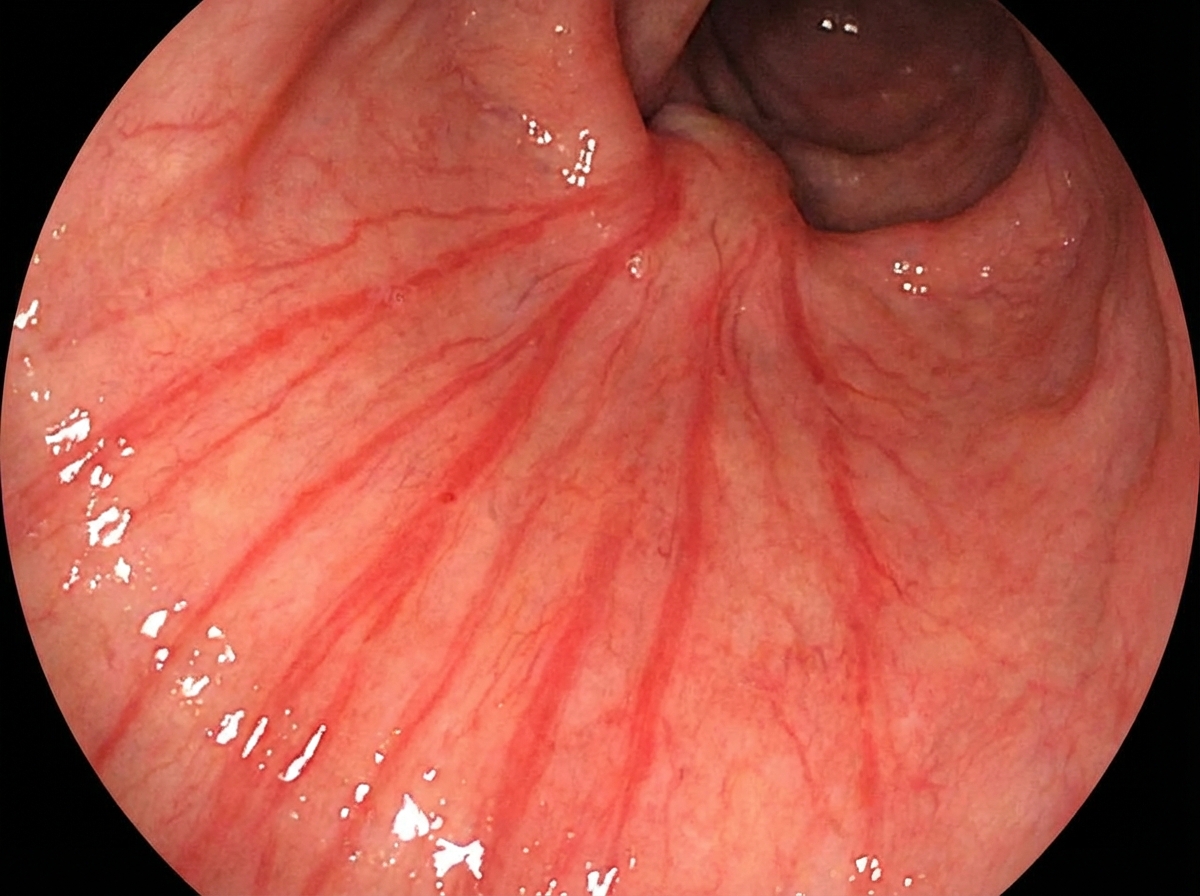
Which of the following conditions leads to the endoscopic appearance shown in the image?
A 65-year-old male presents with abdominal pain and distension. He reports maroon-colored stools and has a past medical history of cerebrovascular accident and myocardial infarction. What is the most probable diagnosis?
A diabetic patient presents with liver cirrhosis and hyperpigmentation. What is the most likely diagnosis?
A 45-year-old male complains of weakness. He is obese, a type 2 diabetic, and hypertensive. General examination reveals hepatomegaly. Icterus is visible on the sclera, and pale coloration of the skin is present. Which of the following liver diseases can be seen in this patient?
Which of the following statements about pleural effusion in cirrhosis is FALSE?
A 62-year-old man is admitted with abdominal pain and weight loss of 5 lb over the past month. He has continued to consume large amounts of rum. Examination reveals icteric sclera. The indirect bilirubin level is 5.6 mg/dL with a total bilirubin of 6 mg/dL. An ultrasound shows a 4-cm pseudocyst. What is the most likely cause of jaundice in a patient with alcoholic pancreatitis?
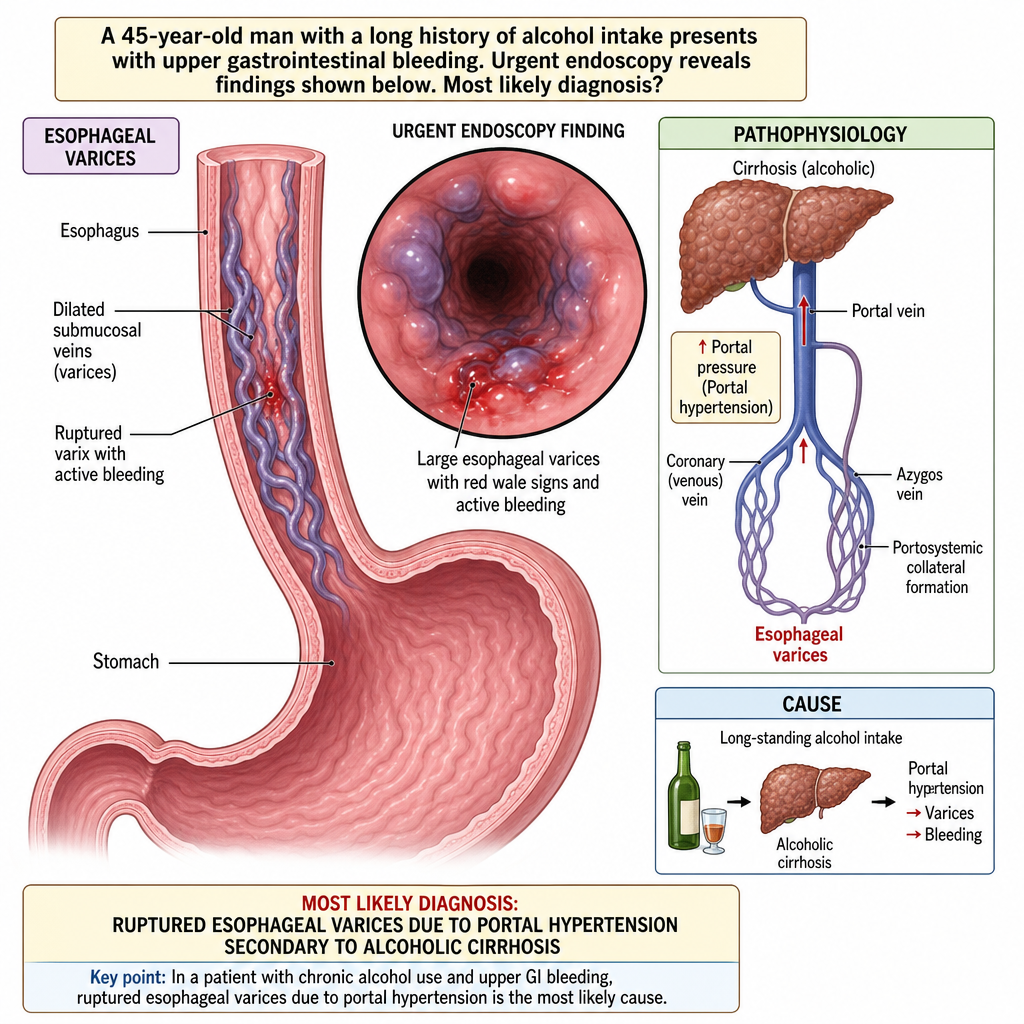
A 45-year-old man with a long history of alcohol intake presents with upper gastrointestinal bleeding. Urgent endoscopy reveals specific findings. Which of the following is the most likely diagnosis?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app