
Gastroenterology — MCQs

On this page
A 25-year-old obese woman who denies any history of alcohol abuse presents with severe abdominal pain radiating to the back. Laboratory results indicate an increase in serum amylase and lipase, with a marked decrease in calcium. Which of the following likely has caused this condition?
Toxic megacolon is seen in -
Portocaval encephalopathy is treated with
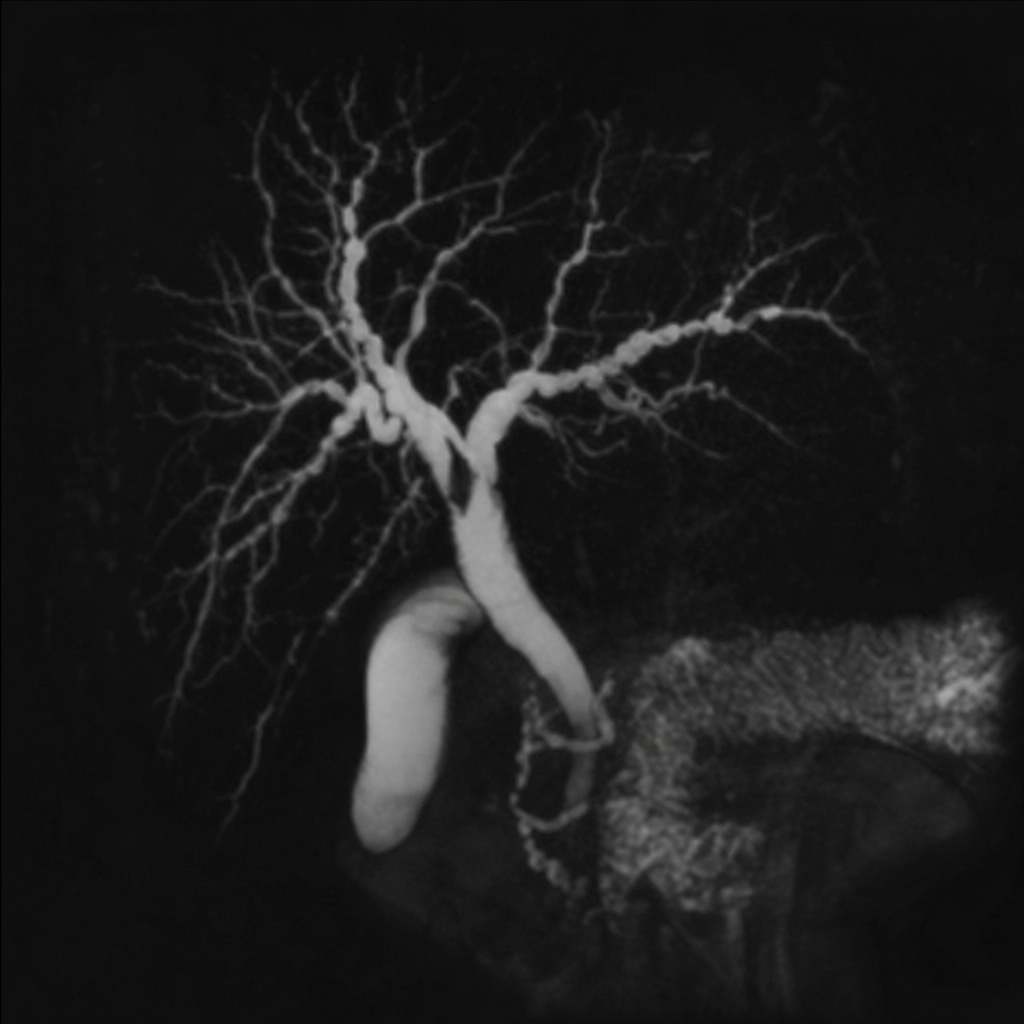
A 35 year old male presenting with recurrent episodes of abdominal pain, jaundice and fatigue underwent MRCP (shown below). What is the most likely diagnosis?
On esophageal manometry, spastic contractions in the esophageal body with a distal contractile integral (DCI) >8000 mmHg*s*cm are diagnostic of:
True statement regarding upper GI bleeds:
All of the following are true about ulcerative colitis except:
Which is the most common site of gastrinoma in MEN 1 syndrome?
What is the differentiating feature between irritable bowel syndrome and inflammatory bowel disease?
What is the Child-Pugh class for a patient who has a serum bilirubin of 2.5 mg/dL, serum albumin of 3 g/dL, INR of 2, mild ascites, but no encephalopathy?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app