
Gastroenterology — MCQs

On this page
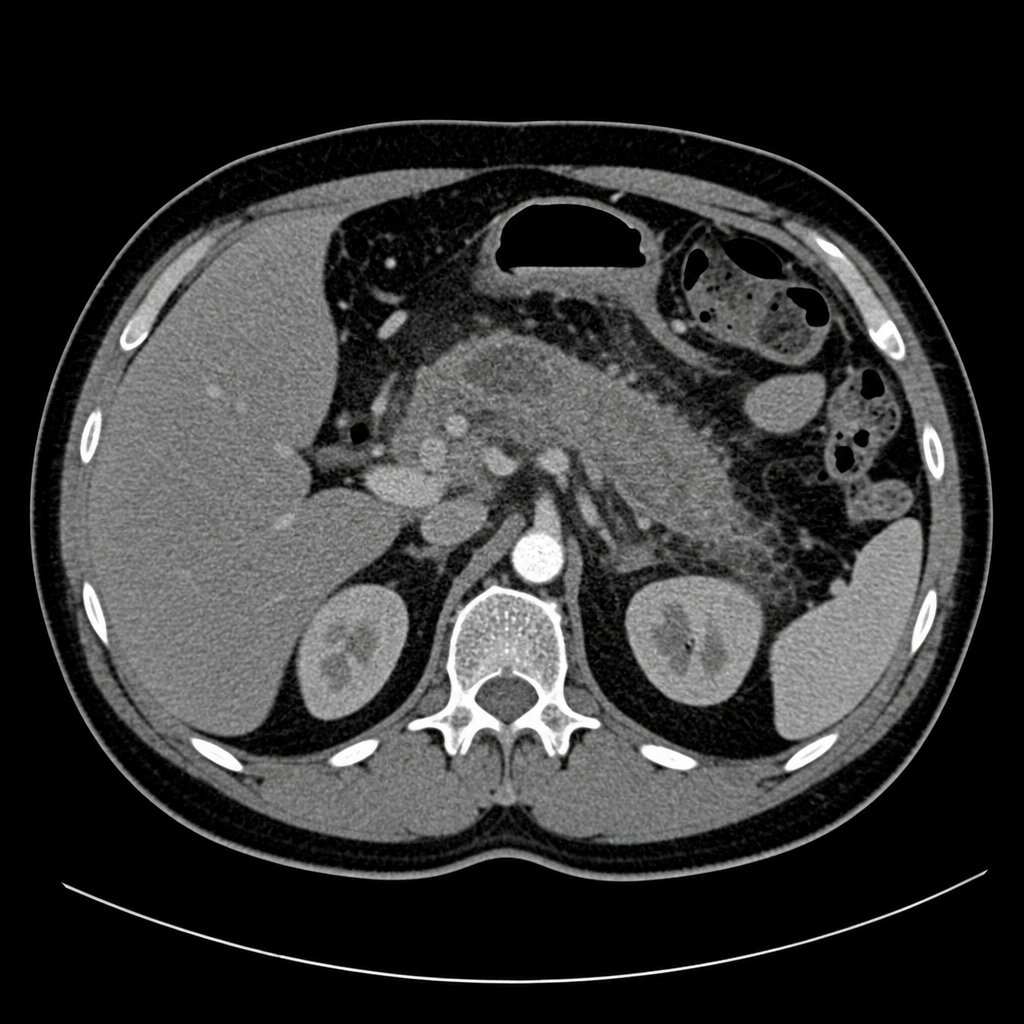
A 60-year-old man is admitted to the ER for a severe persistent abdominal pain of 6 hours duration with nausea, vomiting, and steatorrhea. His medical history is relevant for multiple similar episodes of abdominal pain, hypertension, a recent fasting plasma glucose test of 150 mg/dL, and an HbA1c of 7.8%. His temperature is 37°C (98.6°F), respirations are 15/min, pulse is 67/min, and blood pressure is 122/98 mm Hg. Physical examination is positive for epigastric tenderness. A computed tomography of the abdomen of the patient is shown in the picture, demonstrating findings consistent with chronic pancreatitis (pancreatic calcifications and ductal dilatation), representing an acute-on-chronic pancreatitis presentation. Which of the following laboratory results is most specific for this patient's underlying exocrine pancreatic insufficiency?
True about Crohn's disease except
Which of the following is included in Celiac sprue diet?
Initial treatment for management of mild to moderate Crohn's disease is:
Gold standard method of diagnosing celiac disease is
The highest life time risk of pancreatic malignancy is seen with:
Which of the following is a type of inflammatory bowel disease primarily affecting the small intestine? a) Coeliac disease b) Tropical sprue c) Regional ileitis d) Cystic fibrosis e) Ulcerative colitis
The obstruction of two or more major hepatic veins is seen in:
The most common location of spider nevi is:
All of the following are true about Crohn's disease except.
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app