
Gastroenterology — MCQs

On this page
Which one of the following statements is NOT correct regarding Pyogenic Liver Abscess?
The Child-Turcotte-Pugh (CTP) score for quantifying the severity of chronic liver disease includes all variables EXCEPT:
Following complete ileal and partial jejunal resection, the patient is most likely to have-
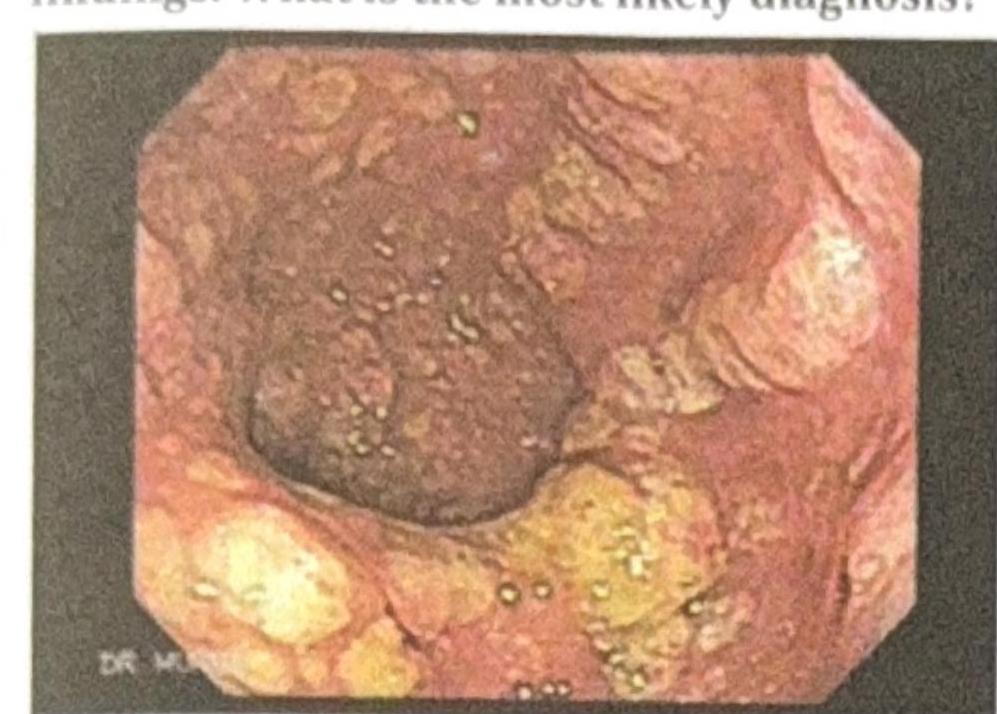
A patient presents to the OPD with recurrent diarrhea, abdominal pain, and foul-smelling stools. The colonoscopy reveals the following findings. What is the most likely diagnosis?
A patient underwent a gastrectomy. Which vitamin replacement is required?
A 24-year-old woman presents to her primary care physician with a longstanding history of diarrhea. She reports recurrent, foul-smelling, loose stools and a 35 lb weight loss over the past 3 years. She also states that two months ago, she developed an "itchy, bumpy" rash on her elbows and forearms which has since resolved. She denies recent camping trips or travel outside of the country. On physical exam she appears thin, her conjunctiva and skin appear pale, and her abdomen is mildly distended. Which of the following tests would confirm this patient's diagnosis?
A 54-year-old man presents to the clinic for epigastric discomfort during the previous month. He states he has not vomited, but reports of having epigastric pain that worsens after most meals. The patient states that his stool “looks black sometimes.” The patient does not report of any weight loss. He has a past medical history of gastroesophageal reflux disease, diabetes mellitus, peptic ulcer disease, and Crohn’s disease. The patient takes over-the-counter ranitidine, and holds prescriptions for metformin and infliximab. The blood pressure is 132/84 mm Hg, the heart rate is 64/min, the respiratory rate is 14/min, and the temperature is 37.3°C (99.1°F). On physical examination, the abdomen is tender to palpation in the epigastric region. Which of the following is the most appropriate next step to accurately determine the diagnosis of this patient?
A 21-year-old woman comes to the physician because of a 2-month history of fatigue, intermittent abdominal pain, and bulky, foul-smelling diarrhea. She has had a 4-kg (8-lb 12-oz) weight loss during this period despite no changes in appetite. Examination of the abdomen shows no abnormalities. Staining of the stool with Sudan III stain shows a large number of red droplets. Which of the following is the most likely underlying cause of this patient’s symptoms?
A 45-year-old woman has a history of mild epigastric pain, which seems to have gotten worse over the last month. Her pain is most severe several hours after a meal and is somewhat relieved with over-the-counter antacids. The patient denies abnormal tastes in her mouth or radiating pain. She does not take any other over-the-counter medications. She denies bleeding, anemia, or unexplained weight loss, and denies a family history of gastrointestinal malignancy. Which of the following is the best next step in the management of this patient?
A 48-year-old Caucasian woman presents to her primary care provider complaining about difficulties while swallowing with fatigability and occasional palpitations for the past few weeks. Her personal history is relevant for bariatric surgery a year ago and a long list of allergies which includes peanuts, penicillin, and milk protein. Physical examination is unremarkable except for pale skin and mucosal surfaces, koilonychia, and glossitis. Which of the following descriptions would you expect to find in an endoscopy?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app