
Gastroenterology — MCQs

On this page
The Model for End Stage Liver Disease (MELD) score includes which of the following variables? 1. Serum bilirubin 2. Serum albumin 3. Serum creatinine 4. International Normalised Ratio (INR)
Among the extra intestinal manifestations of Crohn’s disease which one of the following is related to the disease activity ?
Which of the following statements regarding Ogilvie’s syndrome are correct? 1. It presents as acute large bowel mechanical obstruction 2. Marked caecal dilatation is a common feature on X-ray abdomen 3. Caecal perforation is a well recognized complication of this condition 4. Intravenous Neostigmine is used for the treatment of this condition
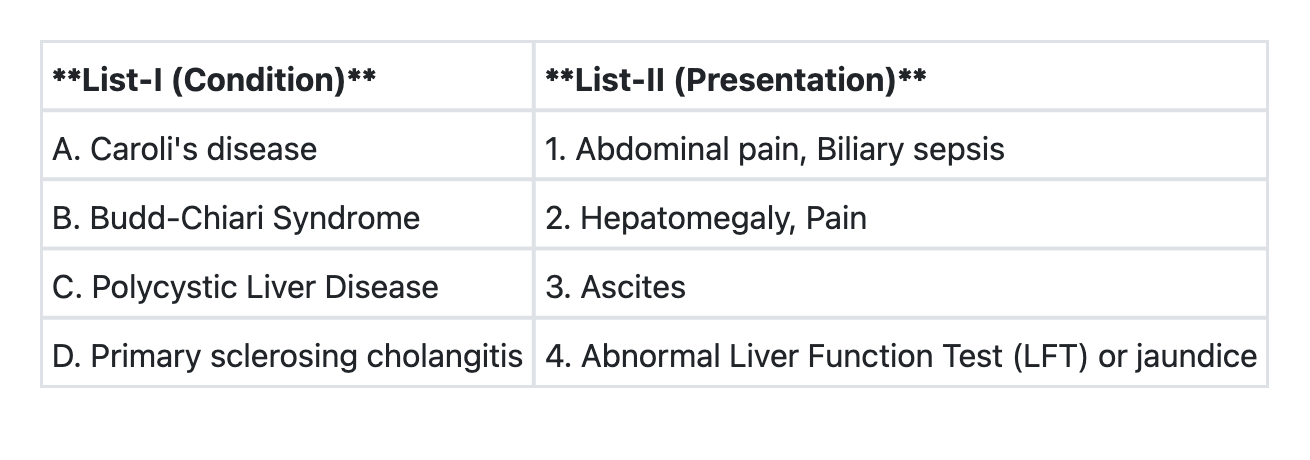
Match List-I with List-II and select the correct answer using the code given below the Lists:
At present, treatment is recommended for H. pylori in association with the following except:
A gentleman of 48 years was being worked up for hepatocellular function. He had no history or signs of encephalopathy. His serum bilirubin was 5 mg%, serum albumin was 3.9 gm%, International normalized ratio was 1.6. On ultrasound no free fluid was detected inside abdomen. As per Child-Turcotte-Pugh (CTP) classification, he was in:
A 40 year old female patient presents with colicky abdominal pain associated with episodes of mild diarrhoea for last 6 months accompanied with intermittent fever and weight loss. There are multiple discharging sinuses on perineal examination. The most likely clinical diagnosis in this patient is:
A gentleman of 36 years presented with a long history of upper abdominal pain which was periodic and often occurred early morning. For last 3 months, he is having projectile vomiting, which is non bilious, unpleasant in nature with undigested food materials. On examination he appears unwell, dehydrated and seemed to have lost weight. Probably he is suffering from:
Spontaneous bacterial peritonitis occurs due to:
Which of the following are correct regarding splenic artery aneurysm? 1. Main arterial trunk is the common site 2. Palpable thrill can be felt 3. It is symptomless unless it ruptures Select the correct answer using the code given below:
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app