
Gastroenterology — MCQs

On this page
A 15-year-old boy presents with abdominal cramps and diarrhea for 8 weeks along with delayed puberty. Perianal examination reveals the following. What is the diagnosis? (NEET Pattern 2018)

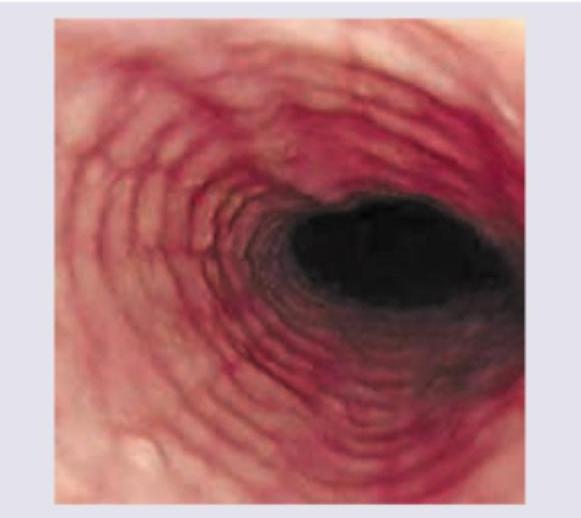
The following appearance of esophagus is seen in:
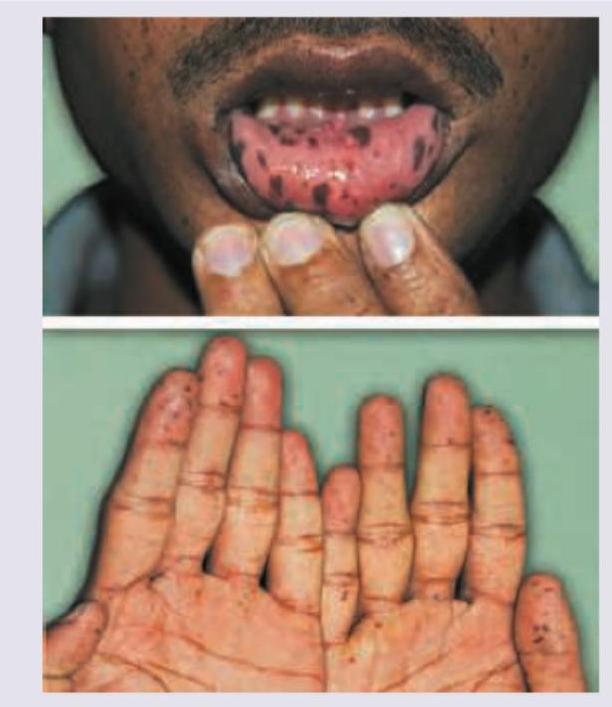
A 20-year-old man with history of melena and abdominal pain has pigmentation of lips. Probable diagnosis is:
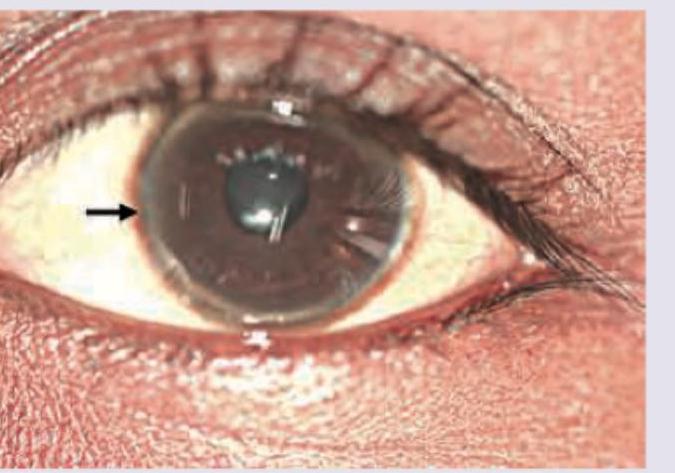
Which of the following is not a component of prognostic index of Nazer in the patient whose naked eye examination is shown below?
Which one of following statements is correct regarding Budd-Chiari Syndrome (BCS)?
Consider the following statements regarding Plummer-Vinson syndrome : I. Findings include cervical oesophageal web, iron deficiency anaemia and dysphagia. II. It is a rare disease, mainly affecting middle-aged women. III. There is predisposition to postcricoid, cervical oesophageal cancer. IV. Treatment is usually surgical. Which of the statements given above are correct?
Which one of the following is considered the gold standard for the diagnosis of oesophageal motility disorders?
A 32 year old man presents with history of recurrent jaundice over the previous decade. Family gives history of the patient having episodes of facial grimacing. Which one of the following is a clinical clue to the diagnosis?
Which one of the following is correctly matched regarding classification of portal hypertension according to site of vascular obstruction?
Which one of the following is a contraindication to wireless capsule endoscopy?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app