
Gastroenterology — MCQs

On this page
A 52-year-old male with chronic hepatitis B presents with progressive abdominal distension and weight loss. Examination reveals ascites and splenomegaly. Serum alpha-fetoprotein is 450 ng/mL (normal <10 ng/mL). Triphasic CT abdomen shows a 6 cm hypervascular lesion in the right lobe with arterial enhancement and washout in portal venous phase. What is the most likely diagnosis?
A male patient presents with chronic diarrhea for 8 months. CT shows ahaustral appearance of the right colon, asymmetric mural thickening, skip lesions with terminal ileal involvement, and creeping fat along the mesenteric border. What is the most likely diagnosis?
The patient presents with fatigue and pruritus. LFT shows gross SALP elevation and elevated conjugated bilirubin. AMA is seen with liver biopsy shows florid bile ductular lesions. Diagnosis is
Based on the image provided, what is the most appropriate confirmatory investigation?
A person with jaundice presented with a history of bleeding and symptoms normalised after giving Vitamin K injection. The probable cause is?
A patient presents with recurrent oral lesions and eye redness as shown in the images below. The patient also reports a diet poor in dairy and meat products and has noticed increased sensitivity to light. Which test is recommended to confirm the suspected nutritional deficiency in this patient?

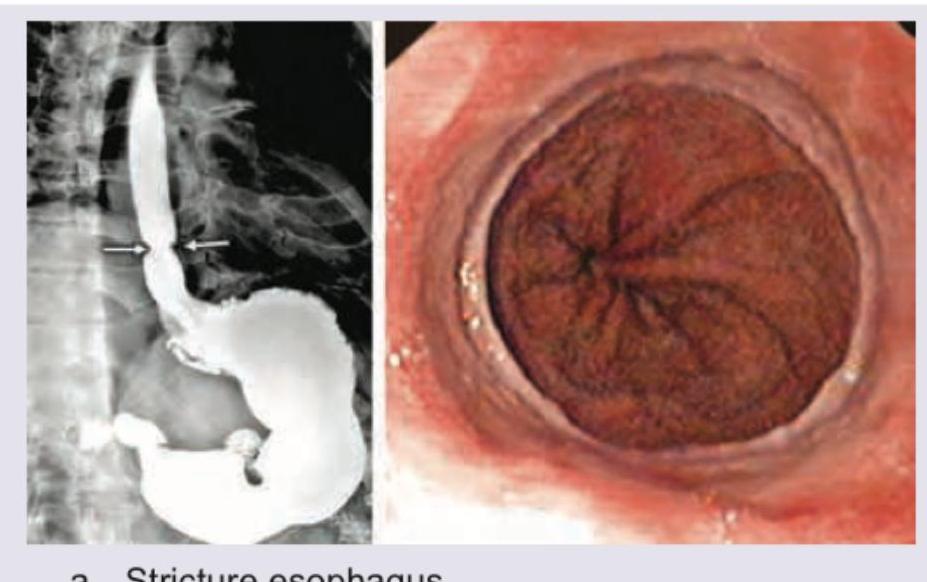
A 42-year-old obese chronic smoker complains of progressive dysphagia to solids, retrosternal heart burn along with sour brash for a period of 6 years. Based on the barium swallow and endoscopic image provided, what is the diagnosis?
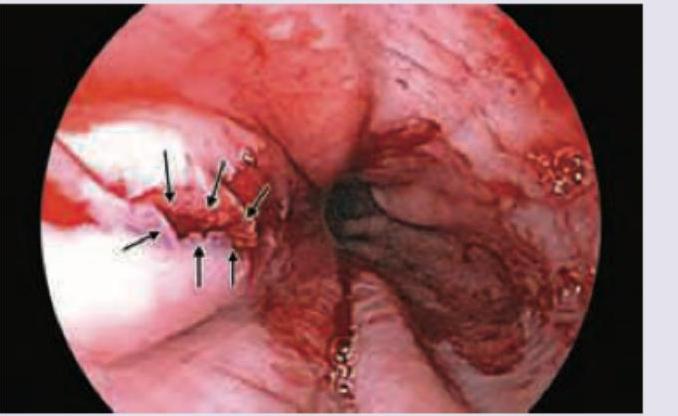
A 28-year-old pregnant female patient complains of hematemesis after an episode of vomiting. On upper GI endoscopy this is the appearance. What is the most common site of this condition?
A 76-year-old male presents to emergency with abdominal pain after binge drinking. The BP on admission is 80/50 mm Hg and pulse rate of 120 BPM. Serum creatinine = 2.5 mg% with elevated liver transaminases. The hypotension and renal failure persisted for more than 48 hours despite adequate resuscitation. What is the likely diagnosis based on CT image shown below? (AlIMS May 2016)

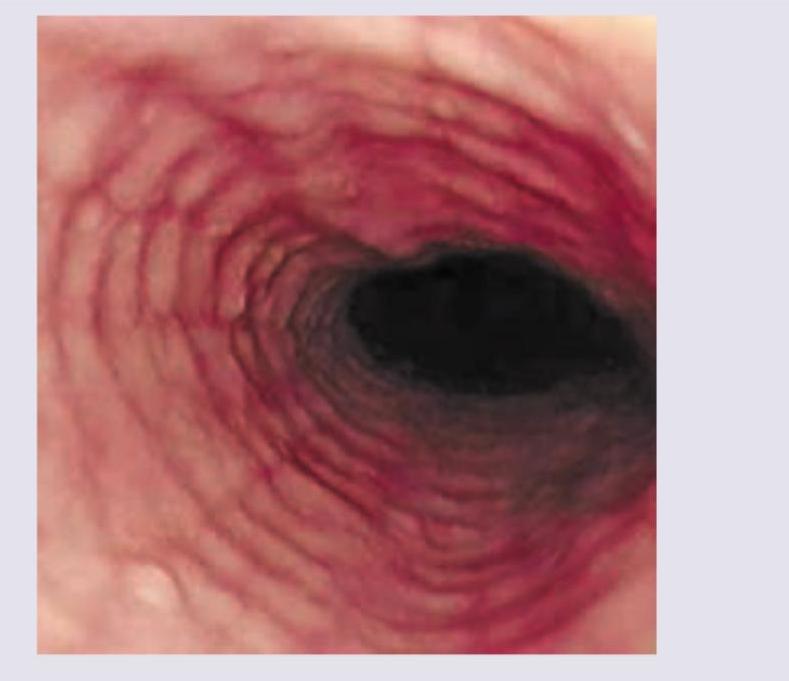
The given endoscopy of the patient shows? (NEET Pattern 2018)
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app