
Gastroenterology — MCQs

On this page
A 19-year-old woman presents with a tremor at rest that has progressively worsened over 6 months. She also exhibits paranoid ideation with auditory hallucinations and has been diagnosed with acute psychosis. Physical examination reveals scleral icterus, and a slit-lamp examination shows corneal Kayser-Fleischer rings. Laboratory findings include total serum protein of 5.9 g/dL, albumin of 3.1 g/dL, total bilirubin of 4.9 mg/dL, direct bilirubin of 3.1 mg/dL, AST of 128 U/L, ALT of 157 U/L, and alkaline phosphatase of 56 U/L. Which of the following additional serologic test findings is most likely to be reported in this patient?
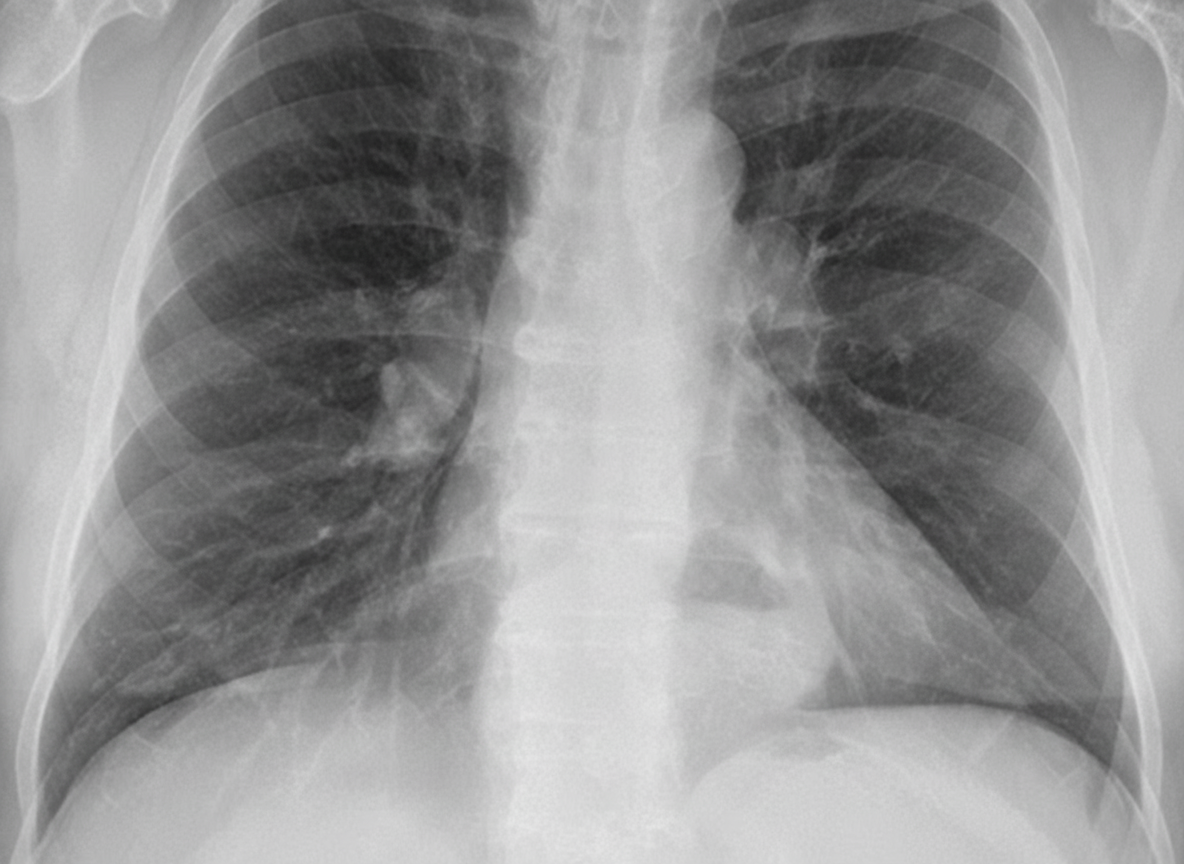
A 64-year-old woman with a longstanding diagnosis of mixed connective tissue disorder and pulmonary fibrosis is admitted with symptoms of recent increase in postprandrial retrosternal distress, heartburn, and nocturnal cough. Her ECG shows nonspecific T-wave changes and she finds minimal relief of her symptoms with sublingual NTG. On examination, she is not in any acute distress and is afebrile. Chest exam reveals bilateral crackles. CXR is shown. What is the most likely cause of this patient's acute symptoms?
According to Child-Pugh criteria, what is the classification for a child with encephalopathy, serum bilirubin of 2.5 mg/dL, serum albumin of 3 gm/dL, prothrombin time of 5 seconds, and controlled ascites?
A 30-year-old woman presents with dysphagia for both solids and liquids. Barium swallow shows a 'parrot beak' appearance. Esophageal manometry reveals increased lower esophageal sphincter (LES) pressure. What is the appropriate management?
Which of the following has the least predilection for the distal ileum?
A young man is brought to casualty with a history of hematemesis and mild splenomegaly on examination. What is the most likely cause of bleeding?
Pruritus precedes jaundice in which of the following conditions?
Palmar erythema is seen in which of the following conditions?
Which one of the following gastrointestinal disorders predisposes to urolithiasis?
What is the best treatment for refractory ascites?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app