
Gastroenterology — MCQs

On this page
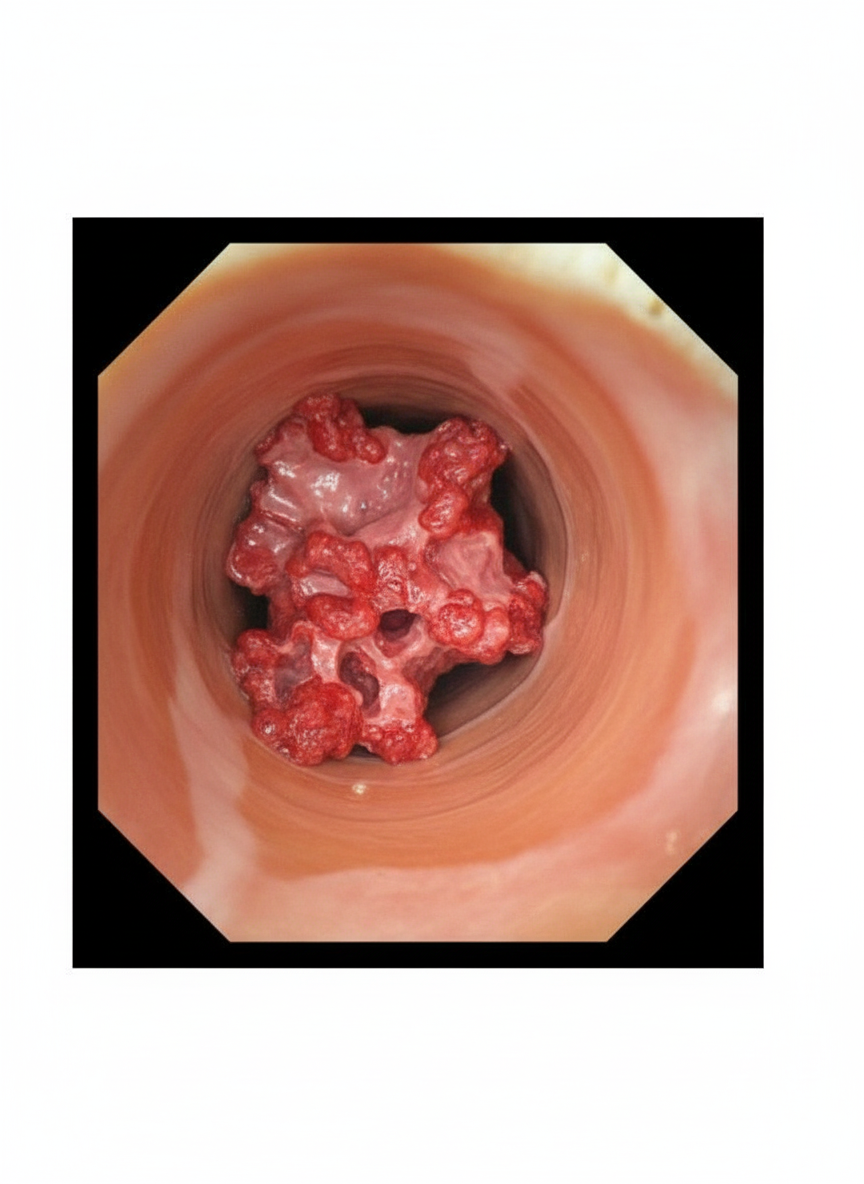
A 58-year-old man with a history of chronic GERD undergoes upper endoscopy. A large, exophytic, fungating mass with irregular borders and friable tissue is found in the distal esophagus. Biopsy reveals glandular differentiation with mucin production. What is the most likely diagnosis?
A 30-year-old male presents with epigastric pain radiating to the back that wakes him up at night and is relieved by consuming food. He has a past history of surgery for a perforated duodenal ulcer, treated with omental patch and proton pump inhibitors and analgesics. What is the likely diagnosis?
The characteristic esophageal manometry finding in achalasia cardia is:
Coomb's positive hemolytic anemia is seen in all of the following conditions except:
Which of the following is NOT a metabolic complication of cirrhosis?
A thirty-year-old male presents to the emergency department with symptoms of epigastric pain radiating to the back. He gives a history of epigastric pain that wakes him up at night and is relieved by consuming food. His past history reveals two episodes of perforated duodenal ulcers which were treated with omental patch surgeries. Pain, before and after the surgery, has been controlled with proton pump inhibitors and analgesics. What is the likely diagnosis on this occasion?
A 26-year-old man presents with intermittent cramping abdominal pain and low-volume diarrhea for 3 weeks. On physical examination, he is afebrile; there is mild lower abdominal tenderness but no masses, and bowel sounds are present. A stool sample is positive for occult blood. The symptoms subside within 1 week. Six months later, abdominal pain recurs with perianal pain. On physical examination, there is now a perirectal fistula. Colonoscopy shows many areas of mucosal edema and ulceration, and some areas that appear normal. Microscopic examination of a biopsy specimen from an ulcerated area shows a patchy acute and chronic inflammatory infiltrate, crypt abscesses, and noncaseating granulomas. Which of the following underlying disease processes best explains these findings?
A 35-year-old lady presented with dysphagia, nocturnal asthma, and weight loss for 6 years. What is the most probable diagnosis?
Dementia is a feature of which disease?
A 29-year-old woman has recently developed milk intolerance. What is the most likely underlying condition?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app