
Gastroenterology — MCQs

On this page
What is the drug of choice for an acute exacerbation of ulcerative colitis?
The modified Mayo score is used in clinical trials to assess the severity of which condition?
What is true about hepatorenal syndrome?
What is the best test for determining the eradication of H. pylori infection?
Which of the following is NOT associated with acute pancreatitis?
What is true about the early stages of GERD?
Which of the following is true regarding Gilbert syndrome?
Primary sclerosing cholangitis is associated with which of the following conditions?
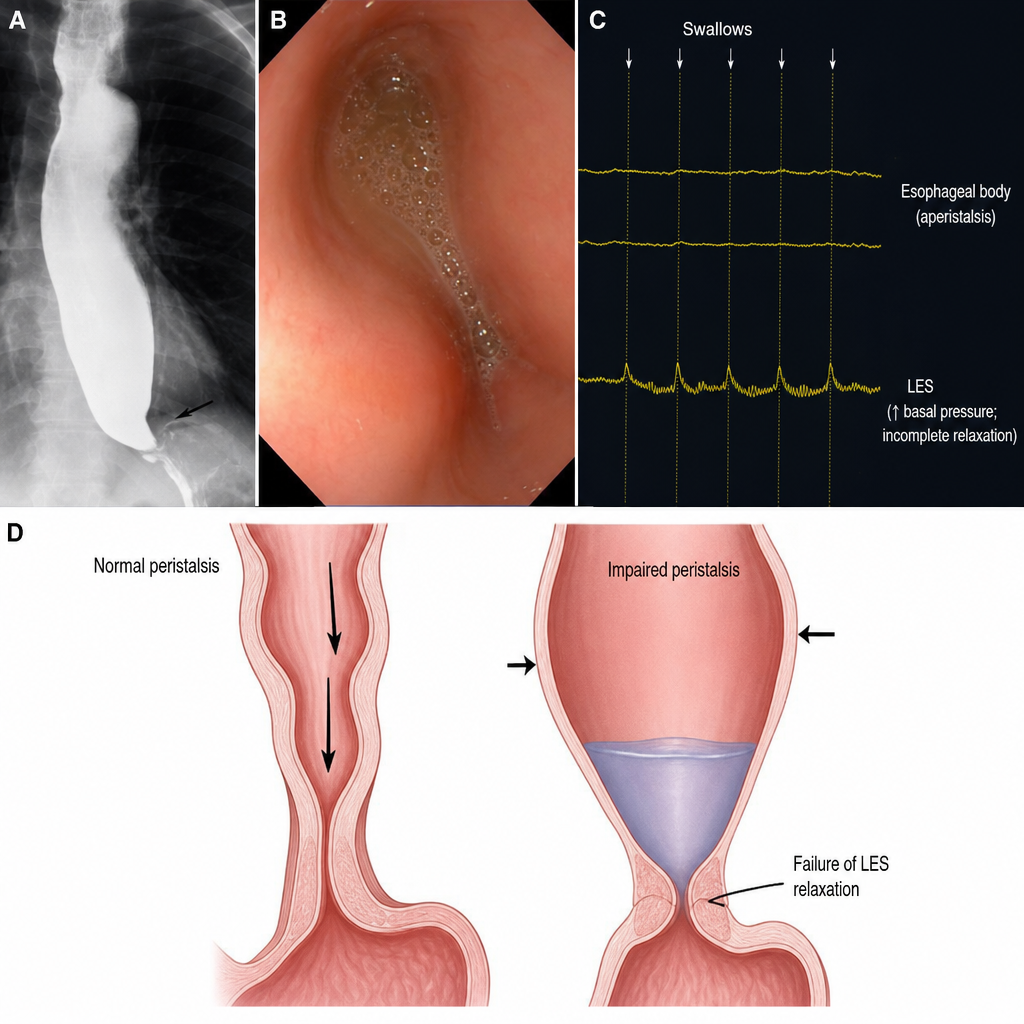
Which of the following statements about achalasia cardia are TRUE? 1. Achalasia results from the degeneration of the myenteric (Auerbach's) plexus and loss of inhibitory nitrergic neurons. 2. Dysphagia in achalasia occurs for both solids and liquids from the onset. 3. Barium swallow showing a "Bird's beak" appearance is the gold standard for diagnosis of achalasia. 4. Manometric findings in achalasia include elevated integrated relaxation pressure (above the manometry system's normative threshold) and aperistalsis in the distal esophagus. 5. Pharmacotherapy with nitrates or calcium channel blockers is the definitive and most effective long-term treatment for achalasia.
Which of the following is a poor prognostic factor in a patient with acute pancreatitis?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app