
Gastroenterology — MCQs

On this page
A 30-year-old male patient with cholelithiasis is found to have serum bilirubin 2.5 mg/dL, Hb 6 g/dL, and urine test positive for urobilinogen. What is the most likely diagnosis?
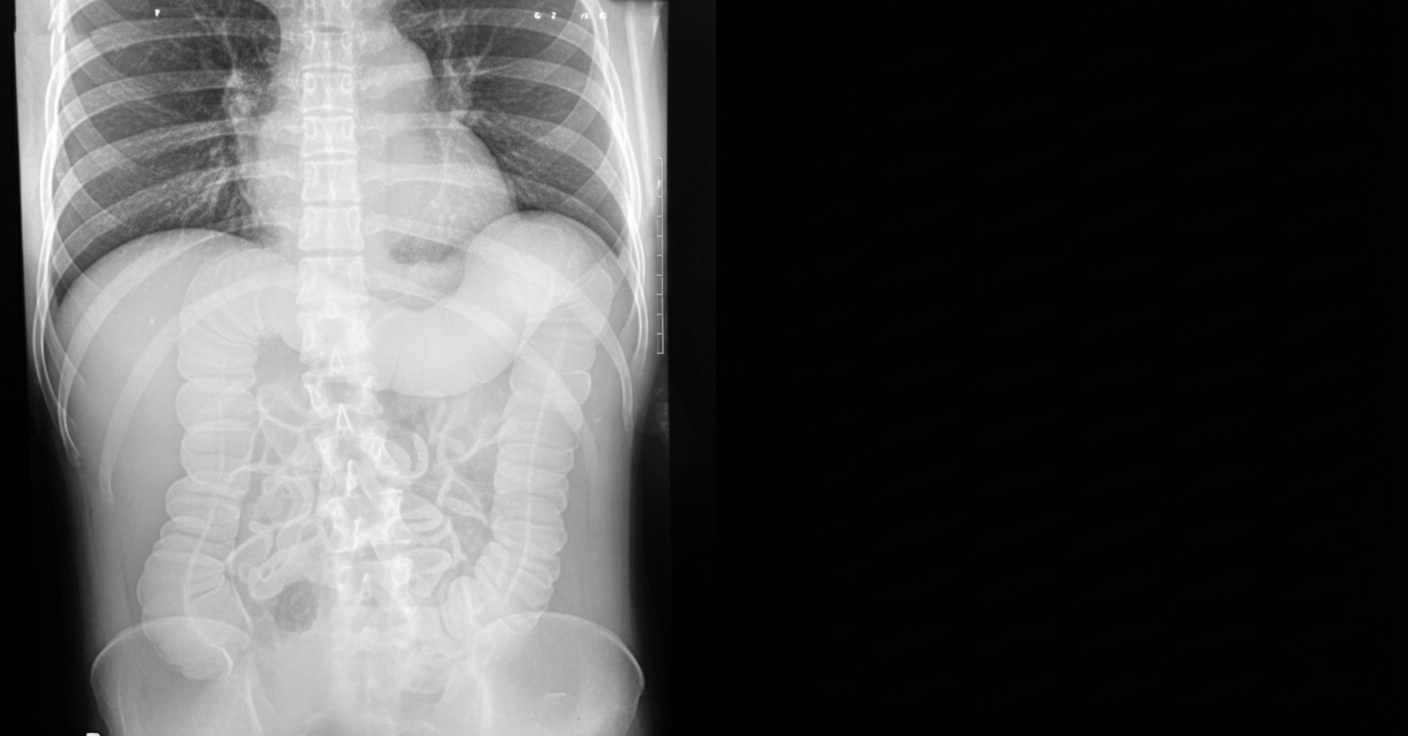
A patient with a known history of ulcerative colitis presents to the emergency department with abdominal distension and tenderness. An abdominal X-ray was performed. Which of the following is true regarding the patient's condition?
A patient presents with upper abdominal pain and vomiting. His pulse is 110/min and BP is 70/40 mm Hg. A diagnosis of pancreatitis is made. What is the next appropriate management?
A 50-year-old lady presented with a history of pain in the upper abdomen, nausea, and decreased appetite for 5 days. She had undergone cholecystectomy 2 years back. Her bilirubin was 10 mg/dl, SGOT 900 IU/L, SGPT 700 IU/L, and serum alkaline phosphatase was 280 IU/L. What is the most likely diagnosis?
Feline esophagus is most commonly associated with which of the following conditions?
Which of the following statements regarding Crohn's disease is correct?
A 25-year-old woman develops nausea, vomiting, and abdominal pain. On examination, she has tender hepatomegaly and ascites. She was recently started on oral contraceptives. What is the most likely clinical diagnosis?
Which one of the following treatments is effective in primary biliary cirrhosis?
What is the best treatment for a refractory peri-anal fistula in Crohn's disease?
Hyper-pigmented skin with xanthelasma and xanthomas suggests the possibility of which diagnosis?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app