
Gastroenterology — MCQs

On this page
Which of the following is considered to be an effective treatment for Type I hepatorenal syndrome?
A patient is found to be positive for HBs Ag on routine laboratory evaluation. Other serological tests for hepatitis are unremarkable. He is clinically asymptomatic and liver enzymes are within the normal range. Which of the following best describes his diagnosis?
A 55-year-old male presents with retrosternal discomfort unrelated to physical exertion. The pain worsens after lying down and is partially relieved by antacids. What is the most likely diagnosis?
A 60-year-old man is found to be disoriented and comatose. He lived alone, ate poorly, and consumed large amounts of hard liquor. Physical examination reveals an emaciated man with a distended abdomen, jaundice, ascites, and a slightly enlarged liver and spleen. Which blood test would confirm a diagnosis of hepatic coma?
A patient presents after setting off a metal detector, despite removing all obvious metallic items. Which of the following conditions could be responsible for this phenomenon?
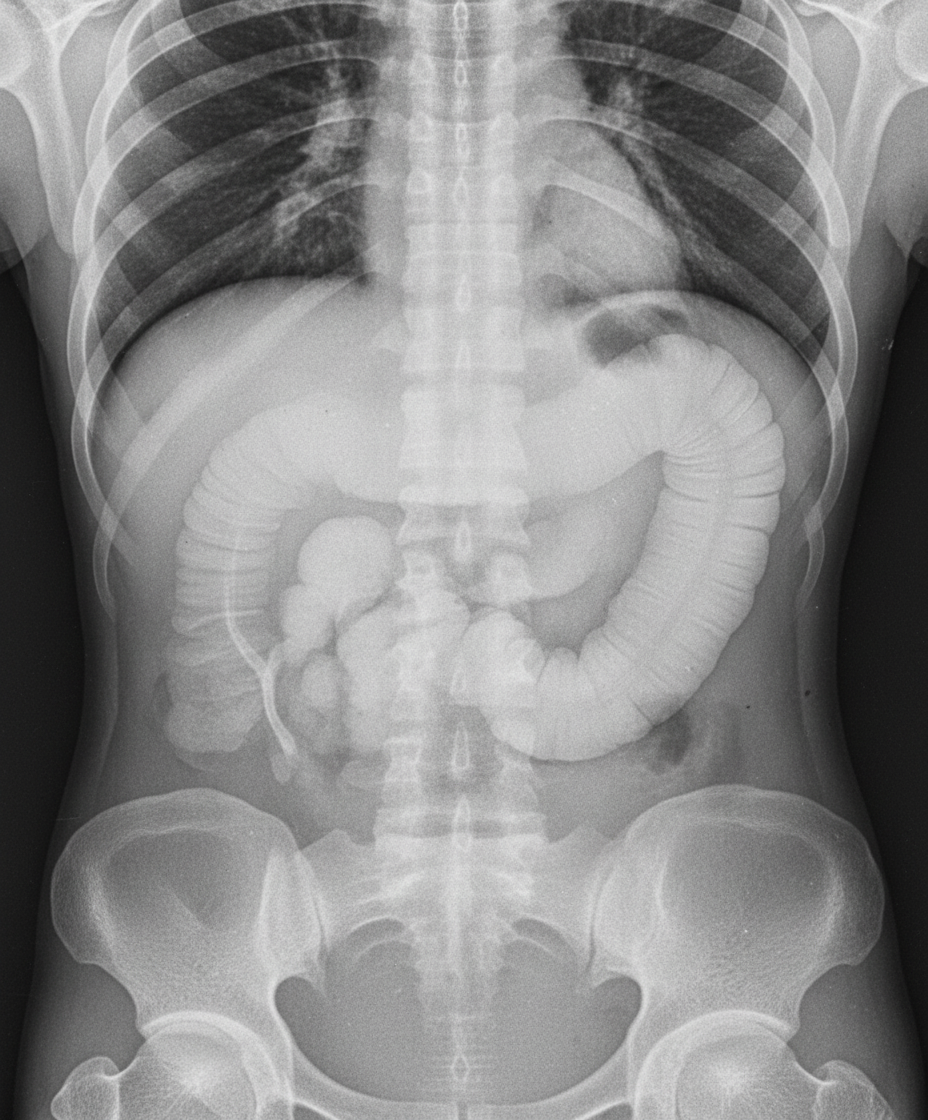
A middle-aged male, a diagnosed case of chronic ulcerative colitis, presents to the emergency department with fever and diarrhea for one week, and acute onset abdominal pain for six hours. An erect abdominal X-ray was taken as shown. What is the likely diagnosis?
A businessman diagnosed with gastroesophageal reflux disease (GERD) presents with substernal heartburn. What is the best test to diagnose GERD and quantify acid output?
A 48-year-old woman presents with severe recurrent peptic ulcer located in the proximal jejunum. Five years previously she underwent parathyroidectomy for hypercalcemia. Her brother was previously diagnosed as having Zollinger-Ellison syndrome. To confirm the diagnosis of Zollinger-Ellison syndrome, blood should be tested for levels of which of the following?
Which test is used to diagnose pancreatic steatorrhea?
Which autoantibodies are seen in type 1 autoimmune hepatitis?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app