
Gastroenterology — MCQs

On this page
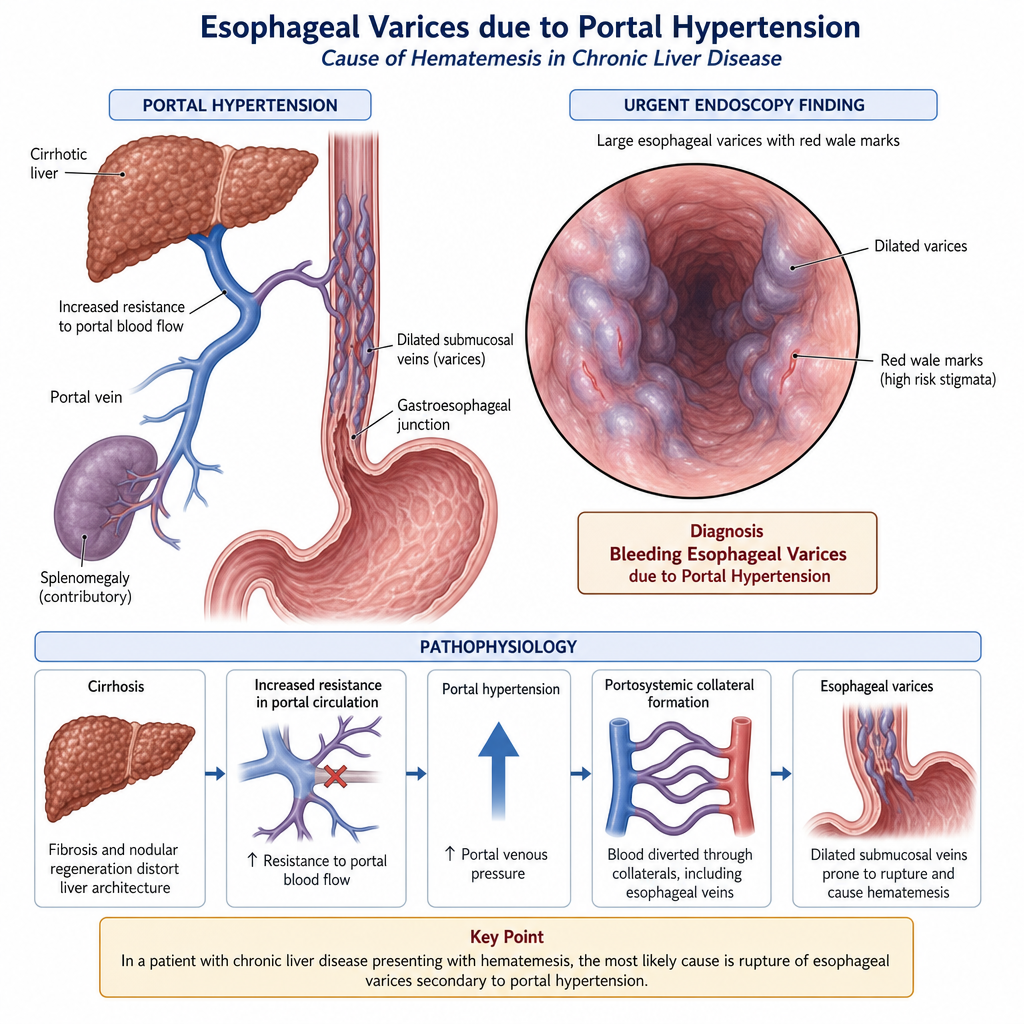
A 50-year-old male presented with a history of hematemesis of 500ml of blood. On examination, his BP was 90/60 mmHg, PR was 110 bpm, and he had splenomegaly 5 cm below the lower costal margin. What is the most probable diagnosis?
Thickened gastric folds are not seen in which of the following conditions?
Which oral lesion is associated with ulcerative colitis?
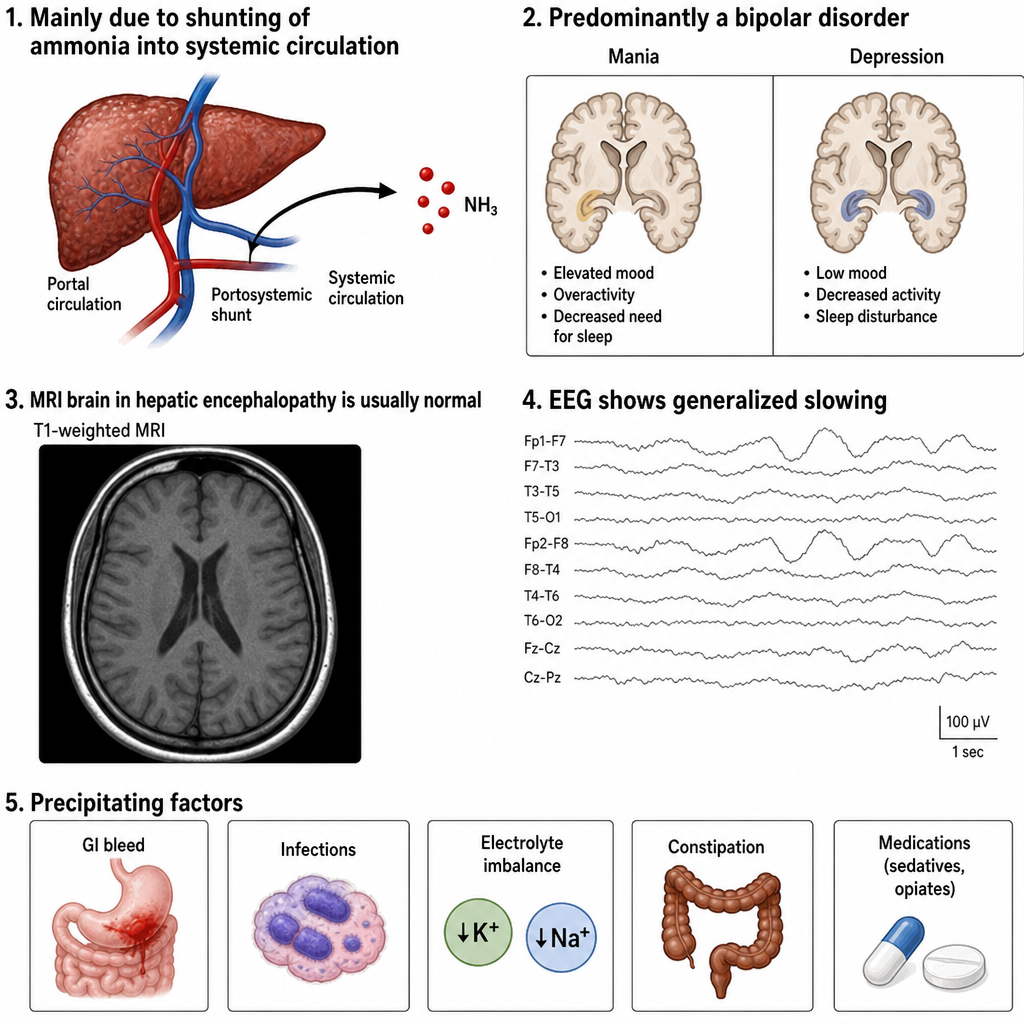
Regarding hepatic encephalopathy, evaluate the following five statements as TRUE or FALSE: Statement 1: Ammonia is the primary toxin implicated in hepatic encephalopathy; it crosses the blood-brain barrier and is converted to glutamine by astrocytes, causing astrocyte swelling. Statement 2: Cerebral edema is a recognised complication of acute hepatic encephalopathy. Statement 3: MRI of the brain in hepatic encephalopathy characteristically shows T1 hyperintensity in the basal ganglia due to manganese deposition. Statement 4: EEG in hepatic encephalopathy characteristically shows generalised slowing of background activity. Statement 5: Gastrointestinal bleeding is one of the most common precipitating factors of hepatic encephalopathy. Which of the following correctly identifies the TRUE and FALSE statements?
A 45-year-old man with a history of chronic alcoholism presents to the emergency department with hematemesis. He denies any prior symptoms of nausea, vomiting, or NSAID use. On examination, his blood pressure is 94/73 mm Hg, heart rate is 110/min, and he has signs of chronic liver disease. Following resuscitation with IV fluids, urgent endoscopy reveals findings suggestive of a specific diagnosis. Which of the following is the most likely diagnosis?
Which of the following conditions does not cause secretory diarrhea?
Non-tropical sprue is characterized by?
Which is the best method for the diagnosis of small intestinal mucosal disease?
A 25-year-old male presents with pigmented macules on his palms, soles, and oral mucosa. He also has anemia and abdominal pain. What is the most probable diagnosis?
A man presents with weakness, pain in the upper abdomen, hyperpigmentation, arthritis, hyperglycemia, and an enlarged palpable liver. What is the most probable diagnosis?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app