
Gastroenterology — MCQs

On this page
Which of the following is associated with Autoimmune hepatitis?
All of the following are important clinical manifestations of hepatocellular carcinoma EXCEPT?
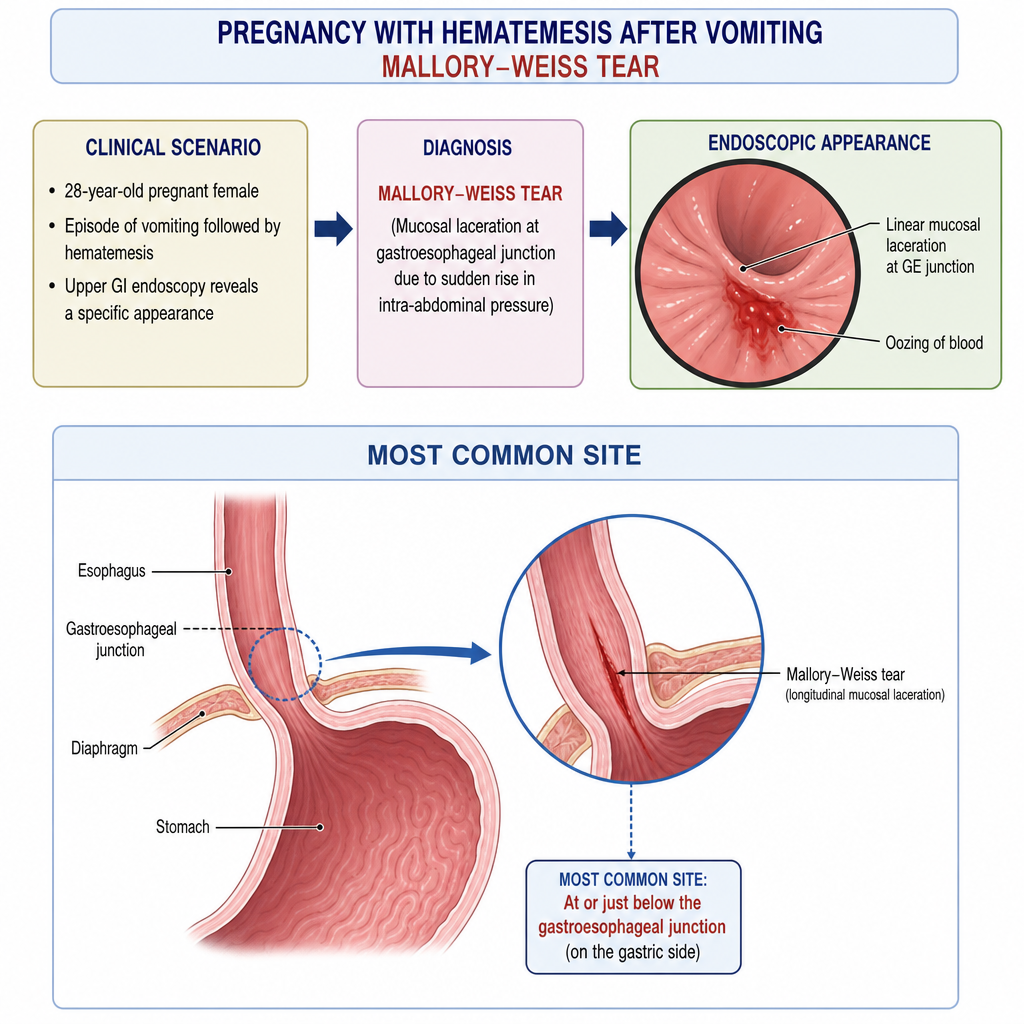
A 28-year-old pregnant female complains of hematemesis after an episode of vomiting. Upper GI endoscopy reveals a specific appearance. What is the most common site of this condition?
What is the first-line treatment for a severe exacerbation of ulcerative colitis?
What is true about ulcerative colitis?
In patients who have undergone appendicectomy, which of the following conditions is less likely to develop?
What is the cause of pruritus in primary biliary cirrhosis?
Colonic pseudo obstruction occurs in all, EXCEPT:
What is the treatment for diffuse esophageal spasm?
What is the best diagnostic test for esophageal motility disorders?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app