
Gastroenterology — MCQs

On this page
Which of the following statements about acute hepatitis is true?
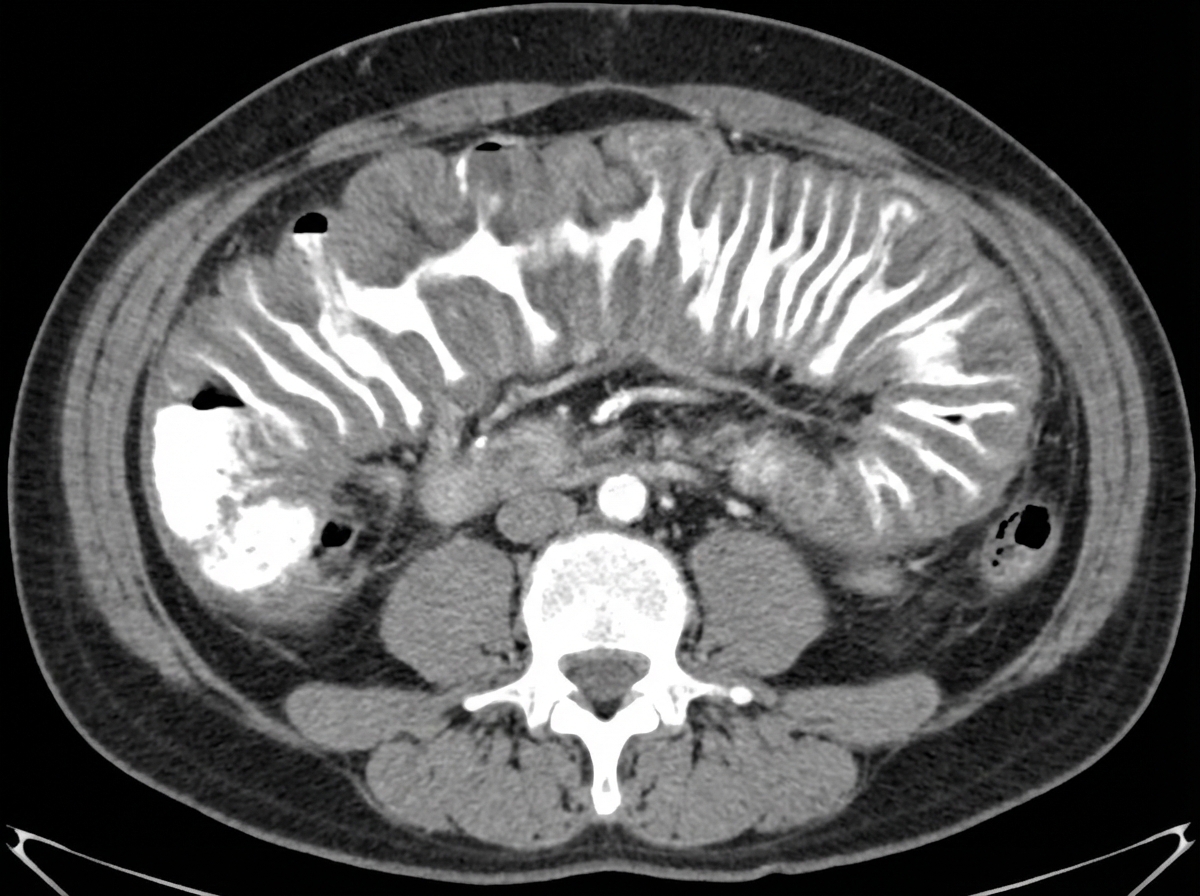
A 40-year-old male presented with watery diarrhea. Stool cytotoxin assay was positive. Colonoscopy revealed ulcers, plaques, and pseudomembranes. The patient's condition improved significantly with metronidazole. The provided CECT shows a characteristic sign. What is the name of this sign seen on CECT?
Poor prognostic factors for acute pancreatitis are all, EXCEPT:
A 52-year-old woman is experiencing abdominal discomfort after meals and early in the morning. She has no weight loss or constitutional symptoms and has tried antacids with minimal relief. Upper endoscopy reveals a duodenal ulcer, and the biopsy is negative for malignancy. What is the most appropriate next step in management?
A 25-year-old man presents with recurrent, indolent fistula in ano. He also reports weight loss, recurrent episodes of diarrhea with blood in the stool, and tenesmus. Proctoscopy reveals a healthy, normal-appearing rectum. What is the most likely diagnosis?
A 60-year-old male presents with progressive difficulty in swallowing, vomiting, and occasional regurgitation for the past 3 months. Barium studies showed marked dilatation of the upper esophagus with narrowing of the lower segment. Manometry showed absent esophageal peristalsis. What is a likely complication this patient would present with?
Zollinger Ellison Syndrome is diagnosed if serum gastrin level is greater than:
A 35-year-old patient has an abnormal Schilling test. After 5 days of antibiotic treatment, the Schilling test normalizes. What is the most likely diagnosis?
A patient presents with esophageal varices and a liver span of 10cm. All of the following are likely causes, except:
What is the most important pathophysiological cause of GERD?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app