
Gastroenterology — MCQs

On this page
Which is the test of choice for assessment of mucosal function of the GIT?
Which of the following is FALSE regarding Primary Sclerosing Cholangitis (PSC)?
What is the first-line treatment for Wilson disease with neurologic or psychiatric manifestations?
Which of the following statements is FALSE about Blind loop syndrome?
A 56-year-old woman with a history of chronic viral hepatitis B and cirrhosis presents with light-headedness upon standing and dark black stools for 3 days. On examination, her blood pressure is 90/60 mm Hg supine and 76/60 mm Hg standing. Abdominal examination reveals distension with ascites, and multiple bruises are noted on her legs. Her laboratory findings include hemoglobin 9.0 g/dL, platelets 90,000/mL, albumin 3 g/dL, bilirubin 1.3 mg/dL, and an international normalized ratio (INR) of 2.5 (prothrombin time 25 seconds). Which of the following coagulation factors are most likely deficient in this patient?
During a routine pre-employment physical examination, an apparently healthy 24-year-old man is found to have increased serum levels of unconjugated bilirubin. Conjugated bilirubin and transaminases are normal. Careful questioning reveals no evidence of recent illnesses. Which of the following is the most likely diagnosis?
A 50-year-old chronic alcoholic and smoker presents with intermittent episodes of epigastric pain, nausea, and vomiting, along with features of malabsorption for the past 6 months. The patient has lost 12 kg over the last year and was hospitalized for acute abdominal pain 3 years ago. Serum amylase and lipase levels are only mildly elevated. A CT scan of the abdomen and MRCP were performed. What is the most likely diagnosis?
A 50-year-old man presented with one episode of hematemesis. On vital examination, HR was 110/min with BP of 110/80 mmHg. Systemic examination shows an enlarged spleen with dilated tortuous veins around the umbilicus. What is the first differential diagnosis?
Heyde's syndrome is characterized by which of the following triad?
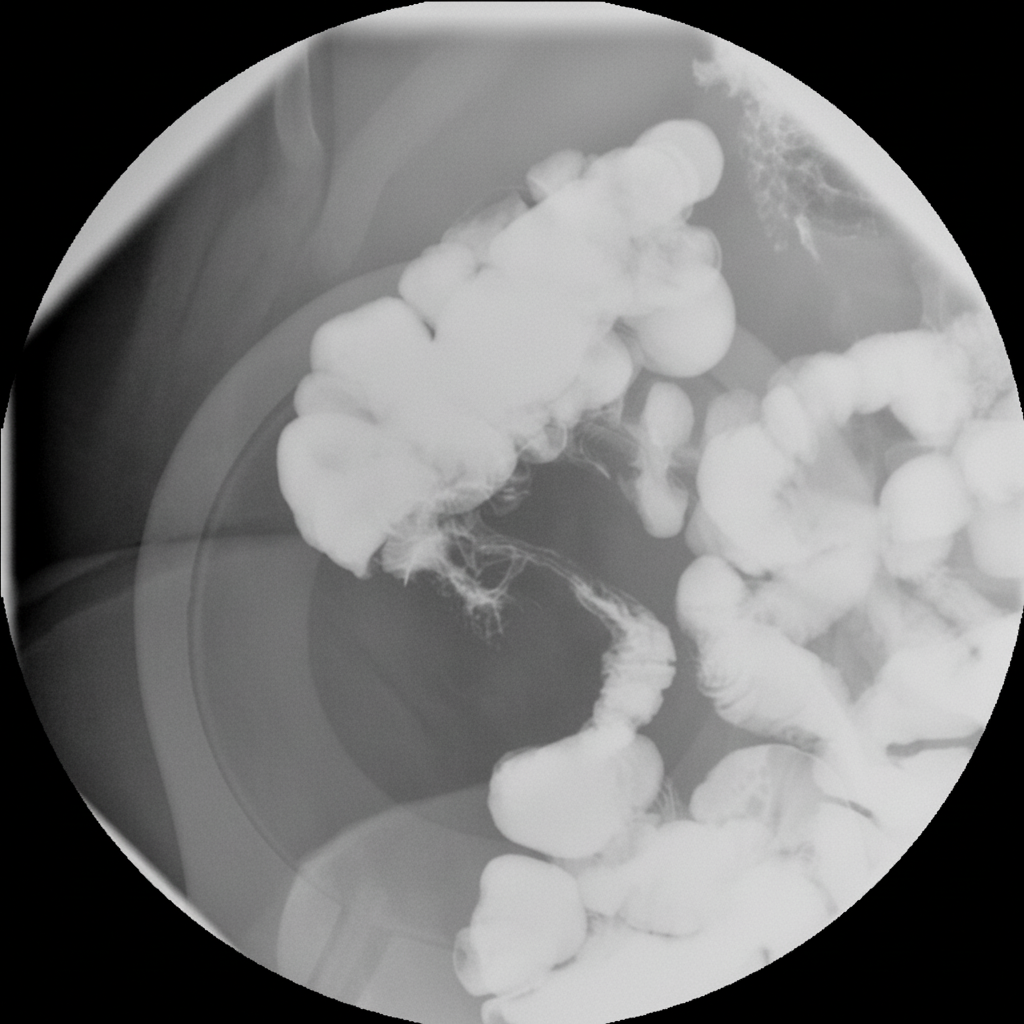
A 32-year-old Caucasian woman with a 12 pack-year history of smoking presents with diarrhea and right lower quadrant colicky pain. Physical examination reveals tender, red nodules on her legs. Radiological examination shows a specific presentation. What is the most likely diagnosis?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app