
Gastroenterology — MCQs

On this page
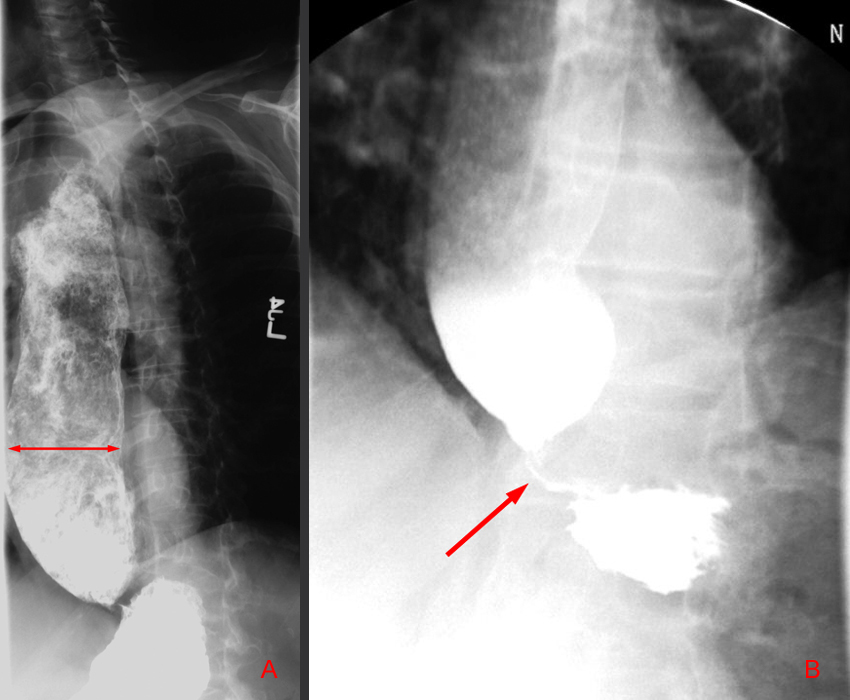
A 50-year-old gynecologist complains of dysphagia, regurgitation, and weight loss, and reports feeling as if food is stuck at the level of the xiphoid. An upright chest X-ray shows a dilated esophagus with an air-fluid level. Which of the following statements is false regarding achalasia?
A 45-year-old man is complaining of vomiting, with vomitus consisting of food mass taken a few days back, foul-smelling breath, and occasional dysphagia to solid food. What is the diagnosis?
Which of the following statements about Hepatocellular carcinoma (HCC) is true?
Urobilinogen levels in obstructed jaundice due to gallstones will be:
Which of the following factors contributes to the formation of cholesterol gallstones?
Which specific condition is a significant risk factor associated with cholangiocarcinoma?
Which of the following factors does not enhance stone formation in the gallbladder?
Increased gastrin is seen in what conditions?
What is the treatment of choice in duodenal ulcer without any complications of hemorrhage?
Which of the following variables is least predictive of 6-week mortality?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app