
Gastroenterology — MCQs

On this page
What is the most common cause of lower gastrointestinal bleeding?
Which of the following is a common cause of acute pancreatitis?
All are true regarding familial adenomatous polyposis except which of the following?
Which of the following conditions is a known precipitating factor for hepatic encephalopathy?
Serum amylase is not raised in
A 60-year-old male experienced a sudden fall in the toilet, with a blood pressure of 90/50 mm Hg and a pulse of 100 beats per minute. His relatives reported that his stool was black or dark in color. Further careful history revealed that he was a known case of hypertension and coronary artery disease, and was regularly taking aspirin, atenolol, and isosorbide dinitrate. What is the most likely diagnosis?
A 45-year-old gentleman has undergone truncal vagotomy and pyloroplasty for bleeding duodenal ulcer seven years ago. Now he has intractable recurrent symptoms of peptic ulcer. All of the following suggest the diagnosis of Zollinger-Ellison syndrome, except:
Which of the following statements about Wilson's disease is true?
Absence of the intrahepatic bile ducts leads to which syndrome?
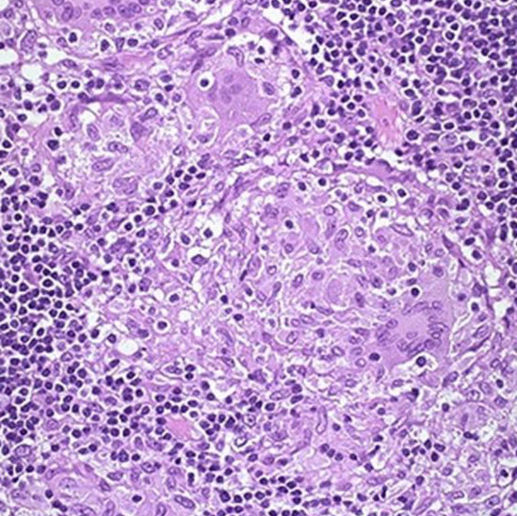
A 40-year-old patient presents with chronic abdominal pain and diarrhea, passing 22-25 stools per day, accompanied by weight loss. On examination, she has mild fever and right lower quadrant tenderness. A lower GI endoscopy reveals the following histopathological findings. An intern in the medicine ward generates a list of differential diagnoses for this patient. Which of the following options is most likely the diagnosis?
Practice by Chapter
Esophageal Disorders
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Irritable Bowel Syndrome
Practice Questions
Malabsorption Syndromes
Practice Questions
Pancreatitis (Acute and Chronic)
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Liver Diseases and Cirrhosis
Practice Questions
Viral Hepatitis
Practice Questions
Biliary Tract Disorders
Practice Questions
Gastrointestinal Motility Disorders
Practice Questions
Gastrointestinal Malignancies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app