
Environmental Medicine — MCQs

On this page
Hyperbaric oxygen is indicated in which of the following conditions?
Severe hypothermia is characterized by all the following EXCEPT:
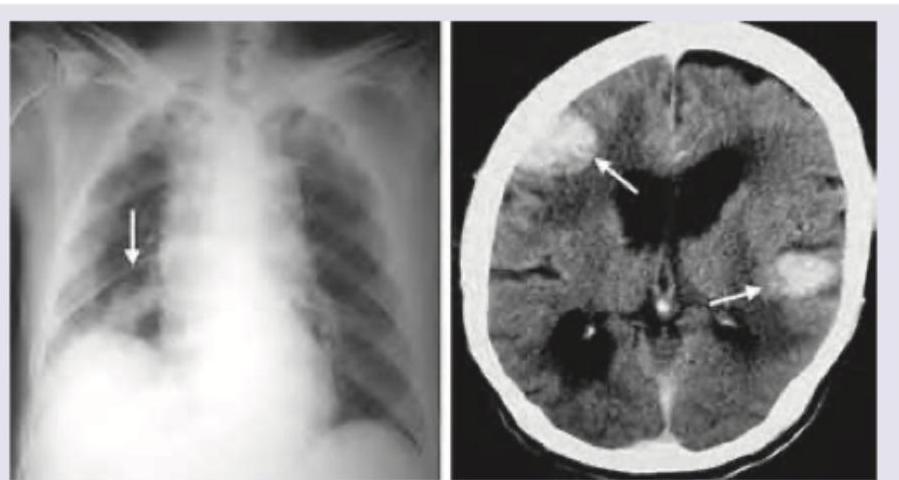
A 65-year-old uranium miner presents with muscle cramps, early morning headache, and serum sodium of 128 mEq/L with serum osmolality of 260 mOsm/kg. Sputum cytology shows small, hyperchromatic cells with scant cytoplasm and nuclear molding. CXR and NCCT scan done shows:
Which of the following is not a feature of heat stress?
A soldier from Siachen came in emergency. How will you rule out hypothermia?
Heat stroke differs from heat cramps or heat exhaustion in that it
A patient aged 24 years is said to have 'severe hypothermia' requiring intensive care management, if his core body temperature is-
Adverse effects of hypothermia are all except:
Which of the following is not done in high altitude sickness?
Which of the following is NOT true about heat stroke?
Practice by Chapter
Heat-Related Illnesses
Practice Questions
Cold-Related Injuries
Practice Questions
High-Altitude Medicine
Practice Questions
Diving and Hyperbaric Medicine
Practice Questions
Radiation Exposure and Safety
Practice Questions
Air Pollution and Respiratory Health
Practice Questions
Water Contamination and Health Effects
Practice Questions
Climate Change and Disease Patterns
Practice Questions
Travel Medicine
Practice Questions
Environmental Allergens
Practice Questions
Disaster Medicine
Practice Questions
Occupational Environmental Hazards
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app