
Edema and Fluid Retention — MCQs

Least common cause for bilateral pedal edema
A patient with heart failure presents with worsening peripheral edema. Which of the following mechanisms contributes most directly to this finding?
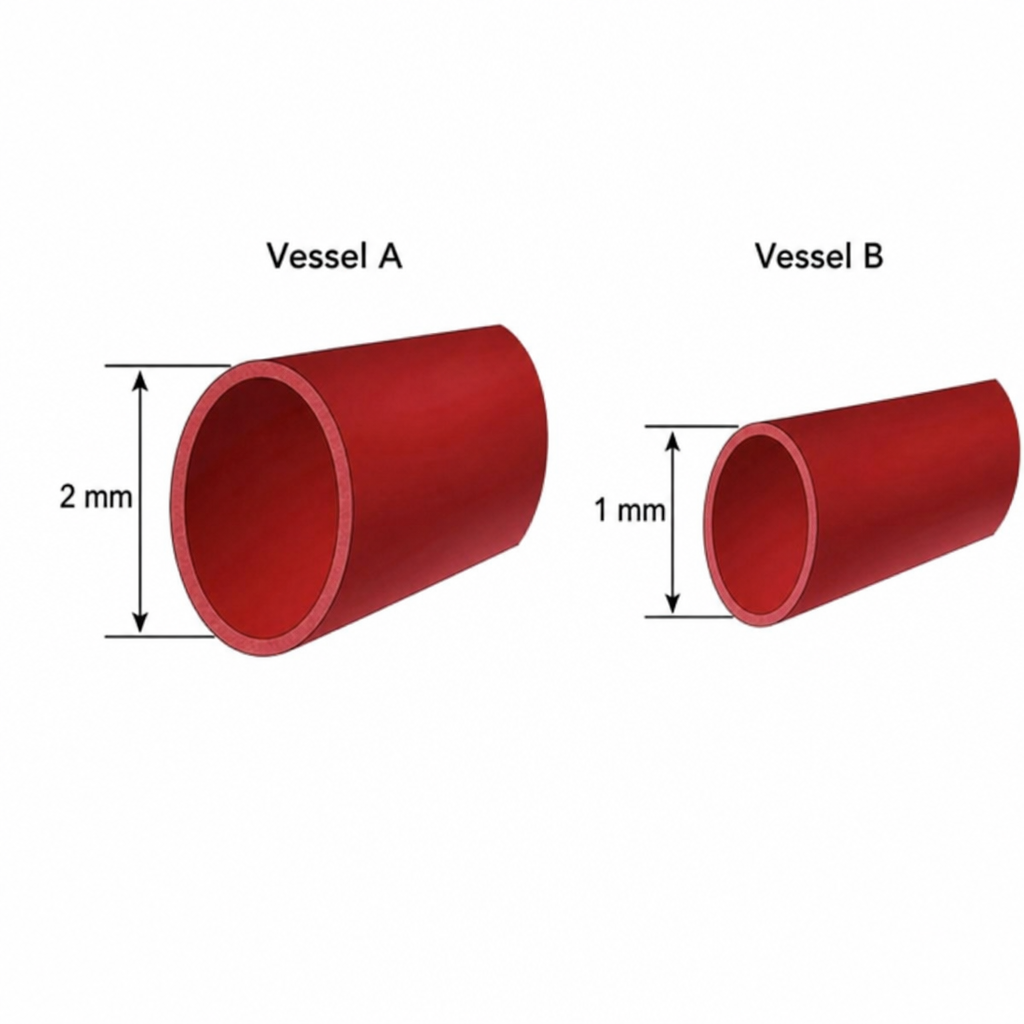
Below are two vessels shown. Assuming the pressure along both the vessels is the same and both of them follow linear flow pattern, what will be the amount of blood flow in vessel A compared to vessel B?
Which condition is most commonly associated with non-pitting edema?
Edema in nephrotic syndrome is due to ?
12 years male came with swelling of lower end tibia which is surrounded by rim of reactive bone. What is most likely diagnosis?
A 40-year-old woman presents with facial swelling, periorbital edema, and proteinuria. Which condition is most likely responsible for her symptoms?
Consider the following clinical features : 1. Raised ICP 2. Seizures 3. Focal deficit 4. Headache Which of the above clinical features are related to most brain tumours?
A 75-year-old man with chronic kidney disease presents with worsening dyspnea and lower extremity edema. Which class of drugs should be used cautiously in this patient?
What is a potential risk associated with the use of thiazolidinediones in the treatment of type 2 diabetes?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app