
Cardiomyopathies — MCQs

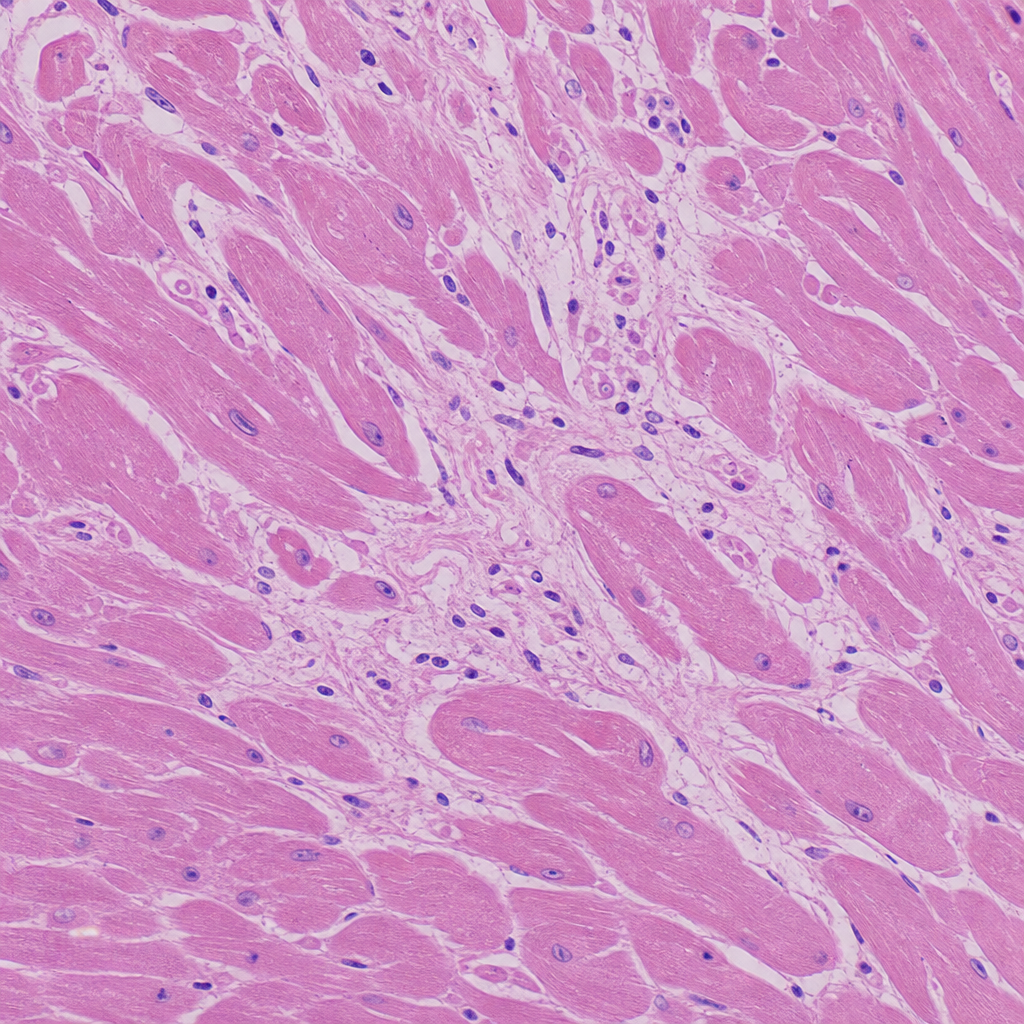
A 30-year-old football player presented to the emergency department with sudden cardiac arrest/collapse. Based on the histological image provided, what is the most likely cause of his death?
A 16-day-old baby girl is brought to the emergency department appearing ill. On examination, she has pallor and dyspnea with a respiratory rate of 85 per minute. Her heart rate is 200 bpm, heart sounds are distant, and a gallop is heard. Chest X-ray shows cardiomegaly. Echocardiogram reveals dilated ventricles and dilation of the left atrium. ECG shows ventricular depolarization complexes with low voltage. What is the most likely underlying diagnosis?
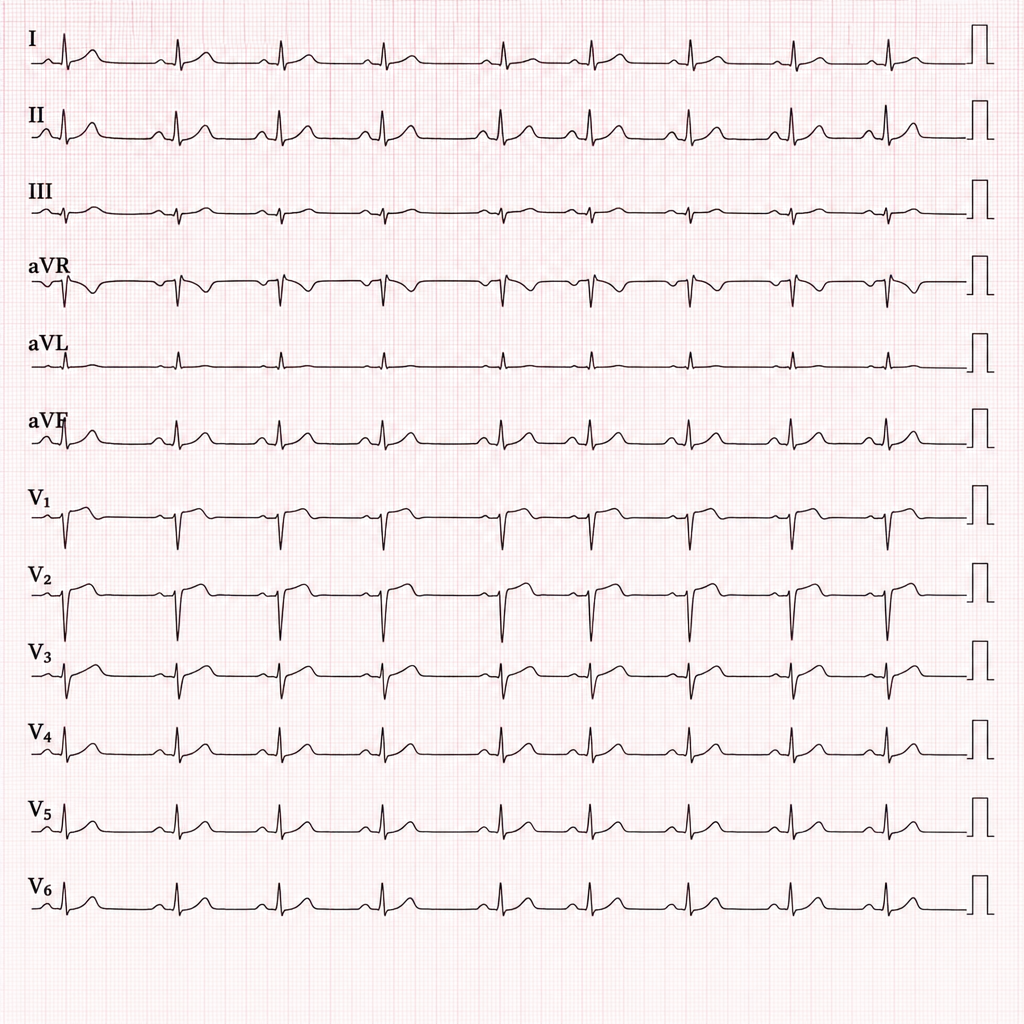
The given ECG shows the following findings:
Which of the following murmur increases on standing?
Which of the following conditions should not be considered if JVP rises on deep inspiration?
Which of the following is NOT a feature of hypertrophic cardiomyopathy on ECHO?
Which of the following is a characteristic hemodynamic finding in pericardial tamponade?
Which murmur increases on standing?
Which condition is suggested by the 'spade-shaped left ventricle' on ECHO?
A man who is chronic alcoholic will develop which type of cardiomyopathy?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app