
General Medicine — MCQs

On this page
A patient presents with the following lesions on the elbows and his blood work shows lactescent plasma. Which is correct about the lesions?

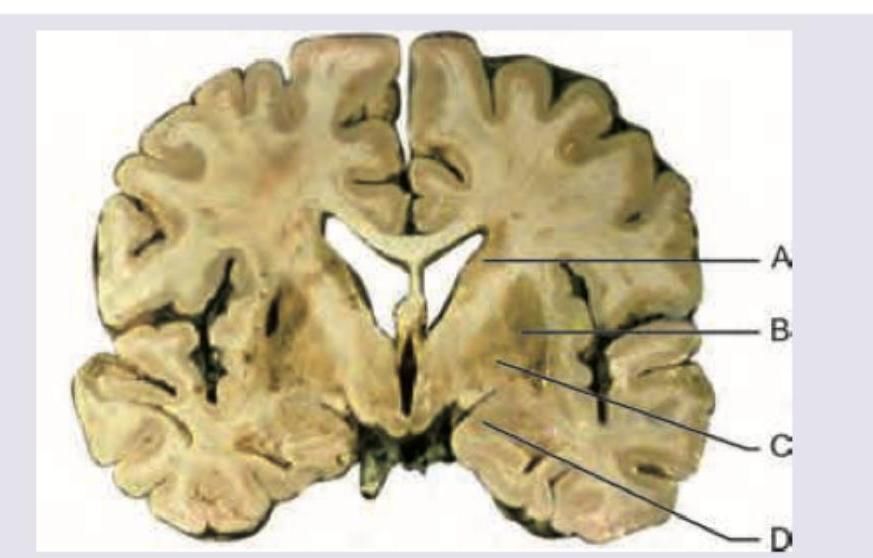
Which of the following is the most common site of hypertensive intraparenchymal bleeding?
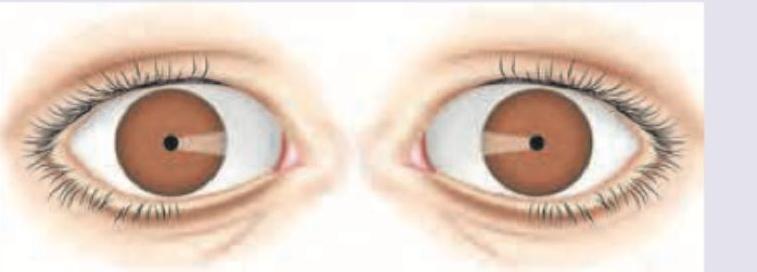
A comatose person is brought to the hospital. On examination his respiratory rate is 8 / min with pulse rate of 75 bpm with BP of 110 / 70 mm Hg. His Pupils are shown below. Body temperature is 96°F. There are no focal neurological deficits. What is the probable diagnosis?
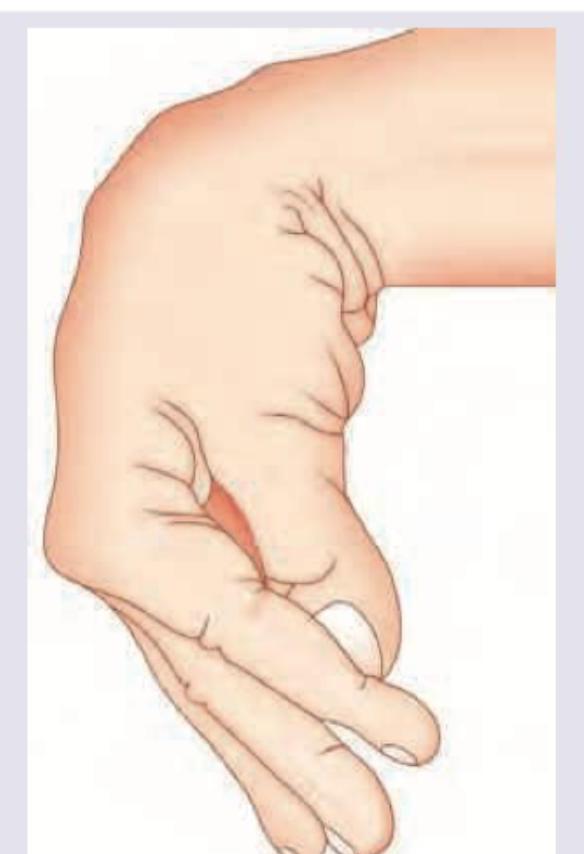
A 65-year-old patient was diagnosed with papillary carcinoma of thyroid. He underwent total thyroidectomy with radical neck dissection. On post-op day 3 he complains of ants crawling sensation on his lips. On deployment of BP cuff in the arm and inflating to 20 mm Hg above SBP, you notice that he develops following posture of his hand. All are true about the condition and its management except:
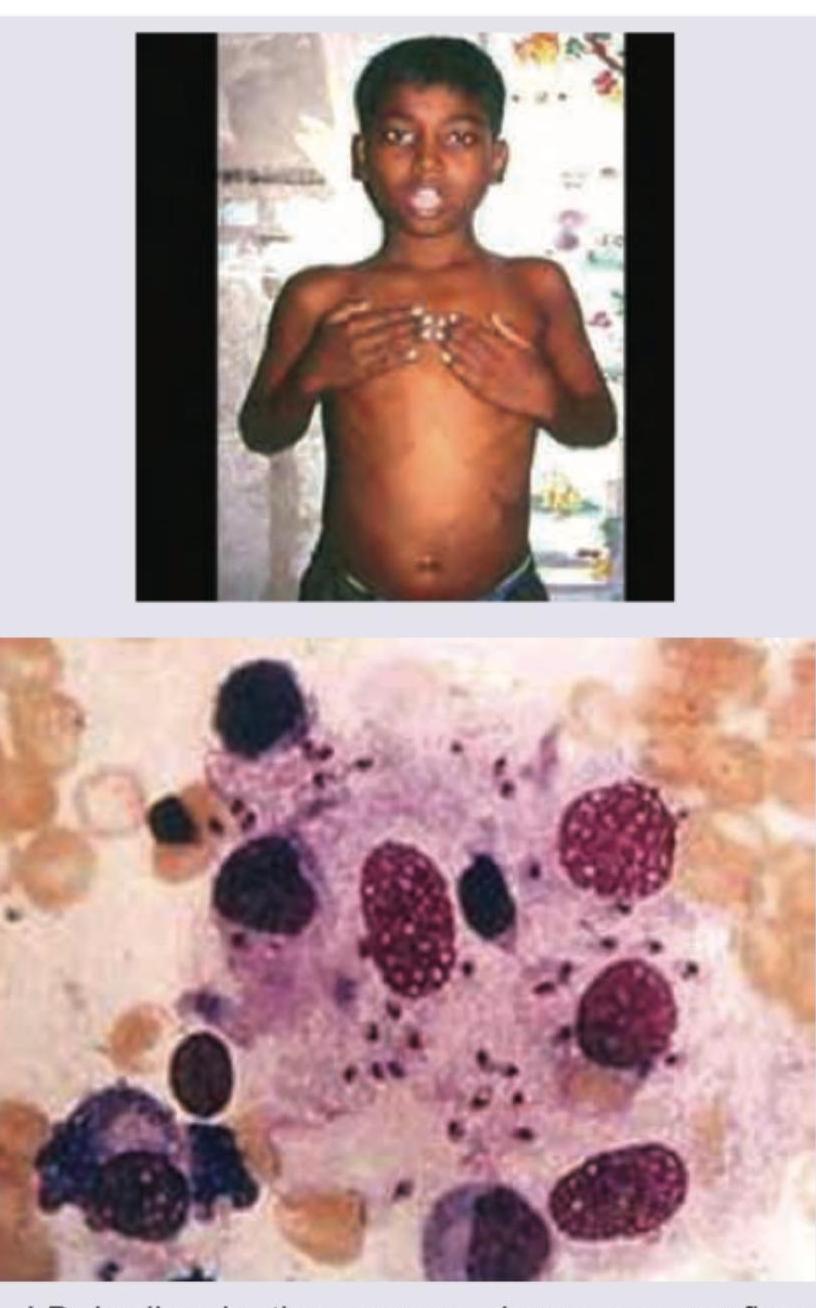
A 8-year-old child from central India presents with fever off and on for last 4 weeks without any chills or rigors. On examination massively enlarged spleen is noted. Bone marrow aspiration was performed. All are correct about the condition shown except:
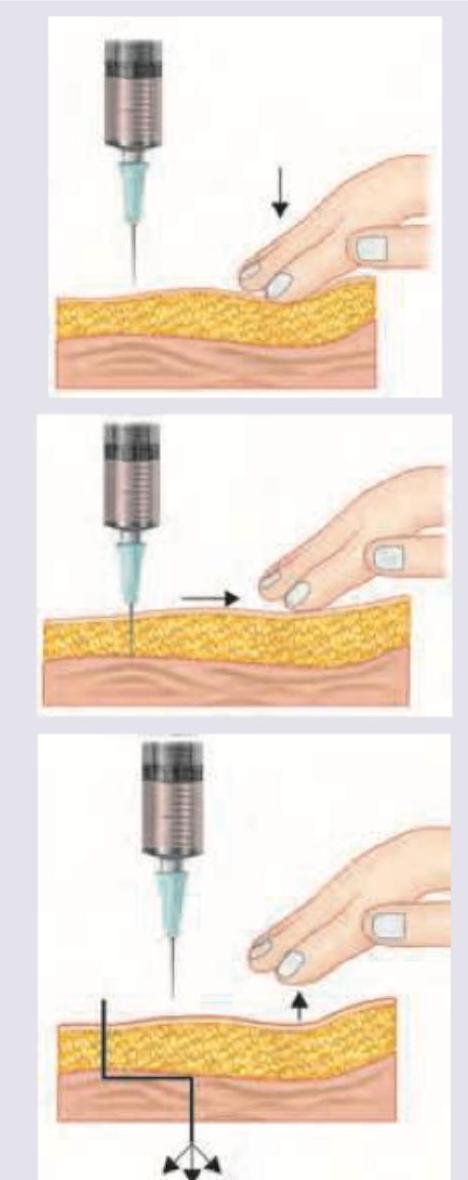
All are correct regarding this technique for administration of intramuscular iron administered by the Z-track technique except:
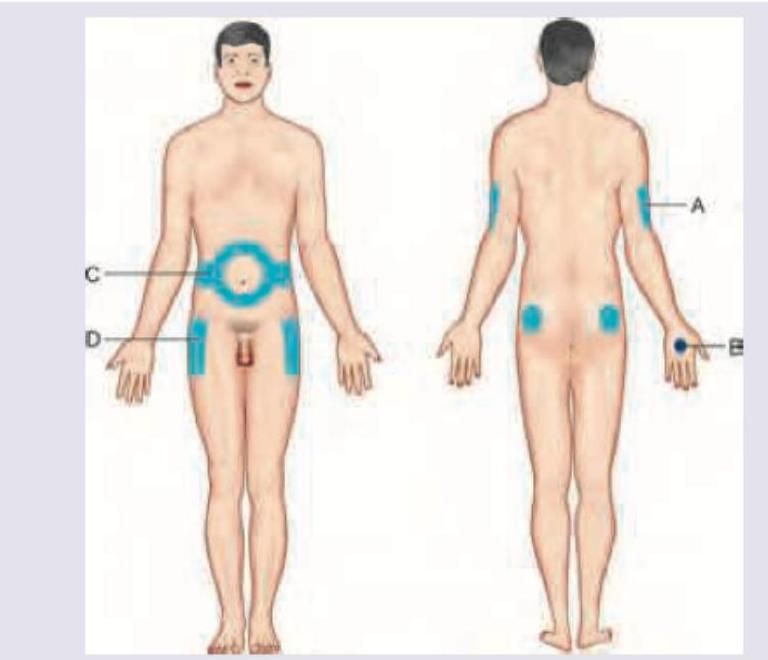
All of the following are sites for giving insulin except:
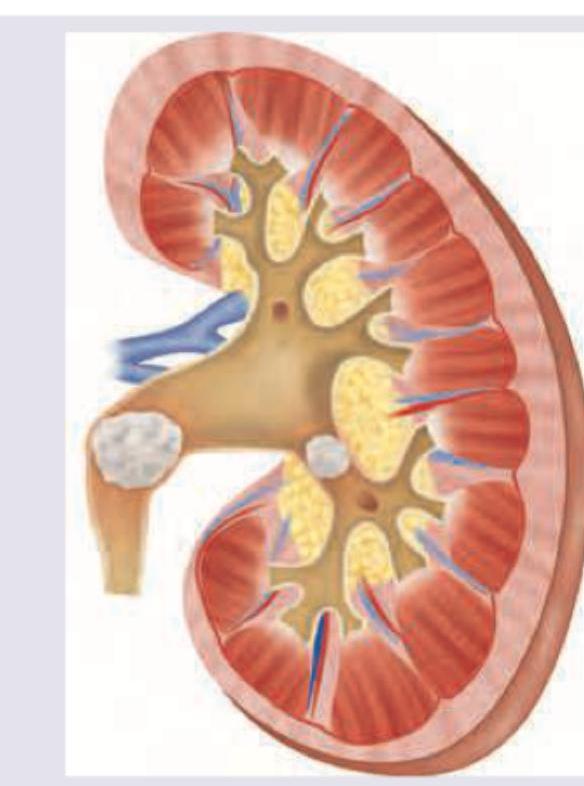
All are correct about the condition shown below except:

A 50-year-old smoker and hypertensive patient presents with the lesion shown below. It is painful and present bilaterally. Peripheral pulses are palpable. What is the diagnosis?

This condition shown below is dependent on development of pH of urine. Which of the following subtype development is insensitive to pH of urine?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app