
Identification — MCQs

On this page
Davidson body is used to determine what about a person?
At what gestational age does the center of ossification of the femur appear?
In fingerprint reader (FINDER) systems, prints of eight fingers are recorded excluding which finger?
Sex differentiation from hair can be made by which characteristic?
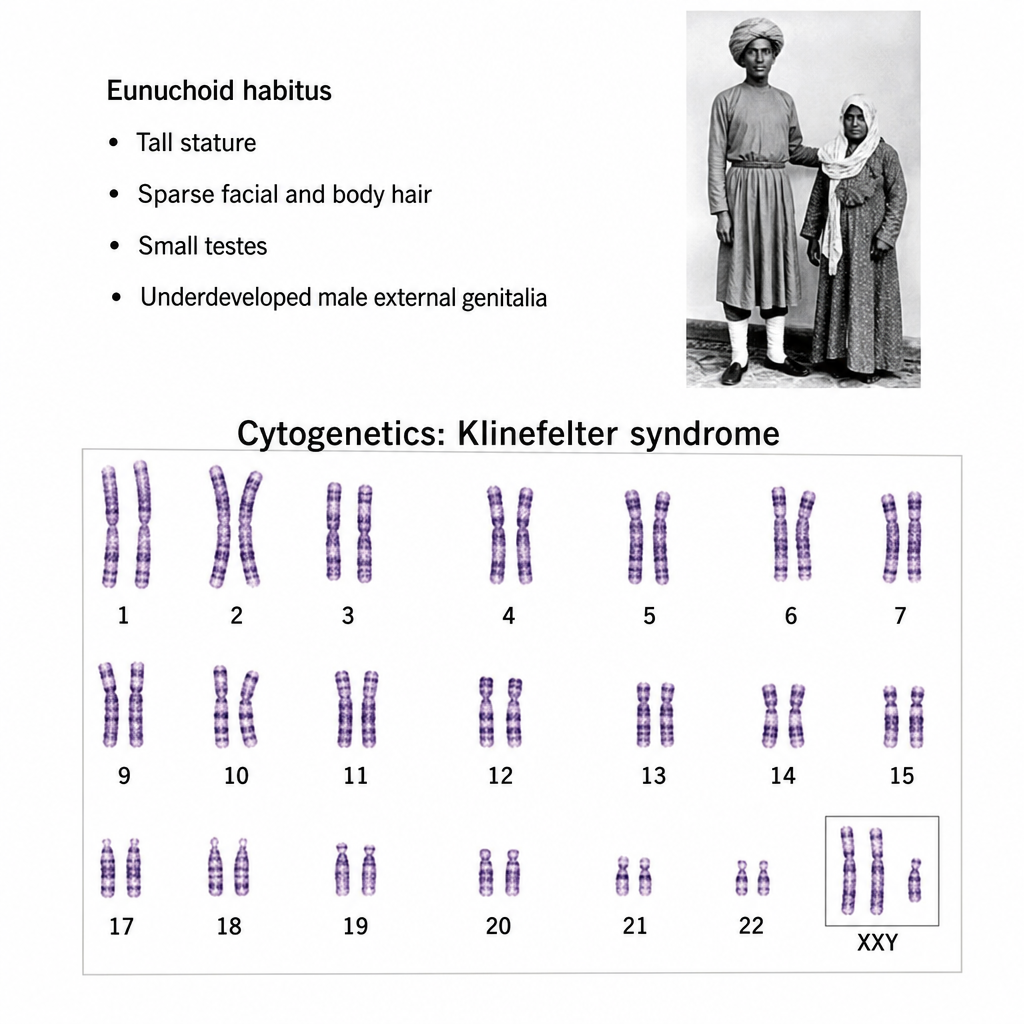
Which of the following statements regarding Eunuchs is true? Statement 1: When castration occurs before puberty, eunuchs show delayed fusion of epiphyses, resulting in eunuchoid proportions (span greater than height; lower segment greater than upper segment). Statement 2: Emasculation (surgical removal of both the penis and testes) constitutes Grievous Hurt under the Indian Penal Code.
Poroscopy in a forensic lab involves which of the following?
A male patient presents for age estimation using the Greulich and Pyle atlas (reference population: North American males). What is the estimated skeletal maturity stage from the given X-ray?

The Singer's Alkali denaturation test is performed to differentiate between:
All of the following statements regarding hair structure and identification are true, EXCEPT?
In the study of latent fingerprints, poroscopy involves which level of detail in individualization on ridge formations?
Practice by Chapter
Personal Identification Methods
Practice Questions
Anthropometry
Practice Questions
Dactylography (Fingerprinting)
Practice Questions
Dental Identification
Practice Questions
DNA Profiling
Practice Questions
Facial Reconstruction
Practice Questions
Superimposition Techniques
Practice Questions
Hair and Fiber Analysis
Practice Questions
Handwriting Analysis
Practice Questions
Identification of Remains
Practice Questions
Mass Disaster Victim Identification
Practice Questions
Age, Sex and Race Determination
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app