
Identification — MCQs

On this page
Identical twins may not have:
What is the most common location for supernumerary teeth?
The sacrum fuses to become a single bone at approximately what age?
Which anatomical feature is most useful for sex determination?
Following the recovery of a skull by the police, the relatives of a missing person want to confirm his identity. Which of the following techniques can be used to figure out a person's identity using the skull and photograph of the person?
A body is found with rigor mortis fully developed in all muscle groups. The ambient temperature is 25°C. Approximately how many hours have elapsed since death?
Which X-ray is used to prove that an individual is more than 18 years of age?
The image shows ossification centers at the lower end of the radius and ulna which are not fused, and the pisiform is present. Based on this, what is the most accurate conclusion about the age?

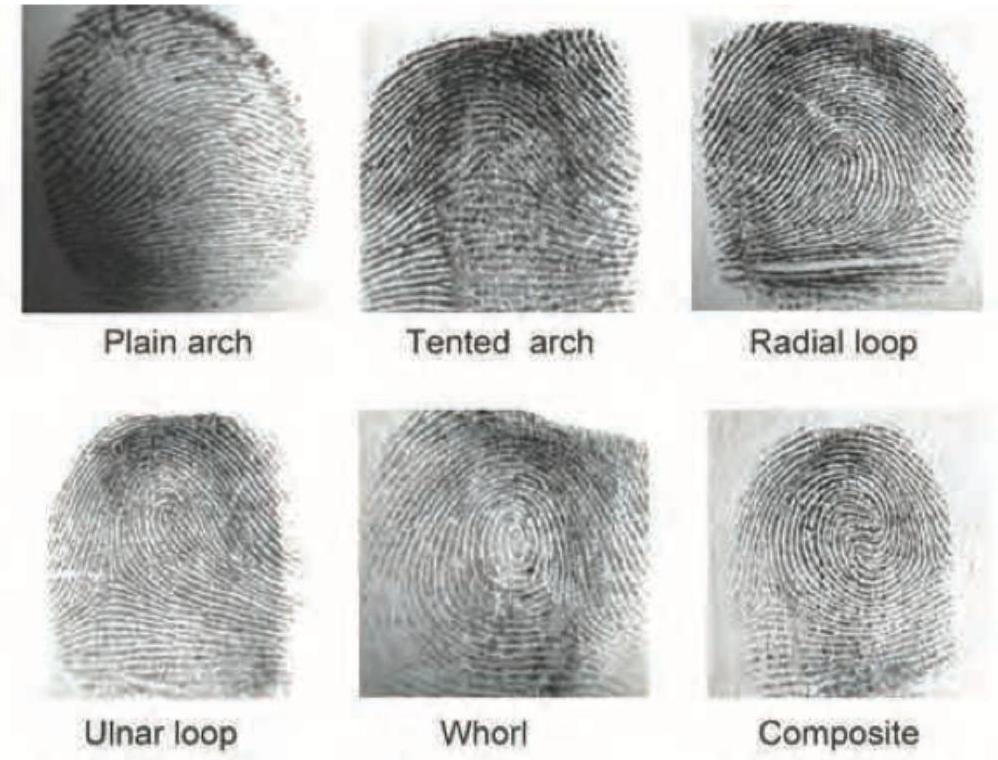
The image shows presence of which pattern? Notice the different patterns shown in the image.
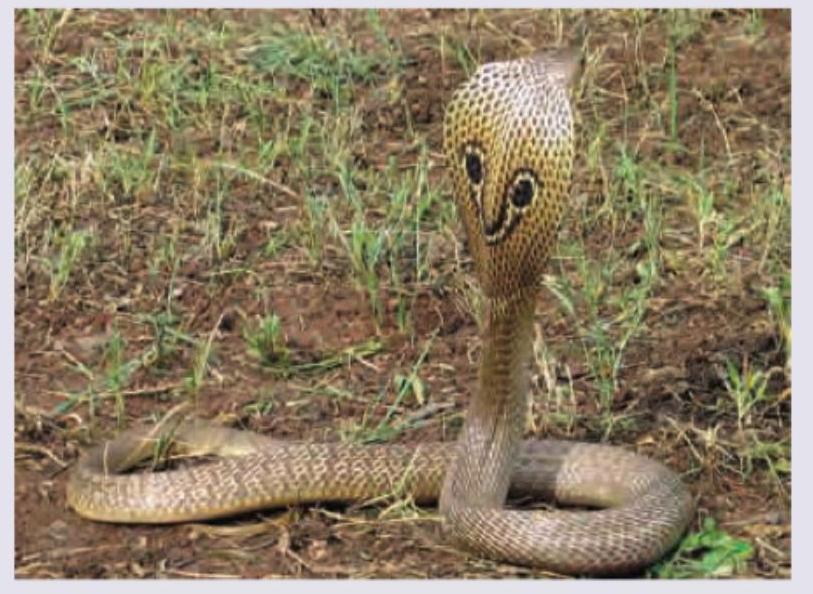
Which snake is shown below?
Practice by Chapter
Personal Identification Methods
Practice Questions
Anthropometry
Practice Questions
Dactylography (Fingerprinting)
Practice Questions
Dental Identification
Practice Questions
DNA Profiling
Practice Questions
Facial Reconstruction
Practice Questions
Superimposition Techniques
Practice Questions
Hair and Fiber Analysis
Practice Questions
Handwriting Analysis
Practice Questions
Identification of Remains
Practice Questions
Mass Disaster Victim Identification
Practice Questions
Age, Sex and Race Determination
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app