
Identification — MCQs

On this page
HLA typing is useful in:
Which of the following is NOT the same in monozygotic twins?
Tattoo is not visible on autopsy. But the presence of tattoo was informed by relative. What is the next site to check?
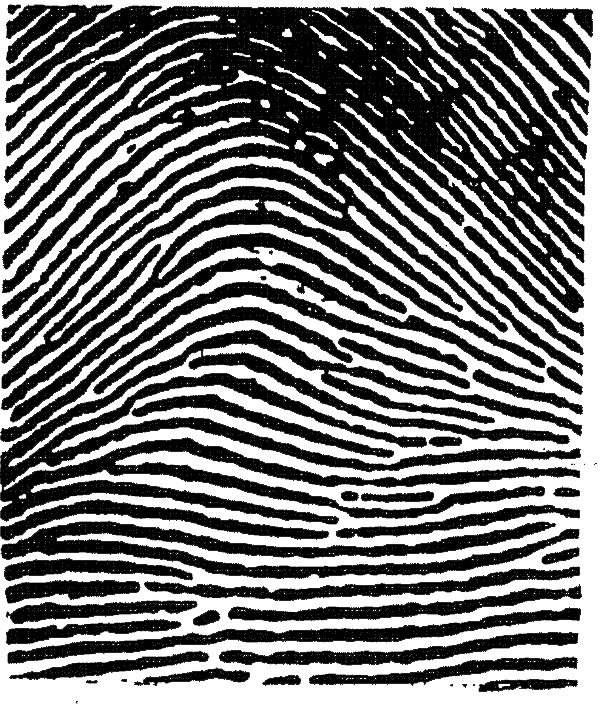
The pattern of fingerprint demonstrated here is
The center of ossification used as medico-legal evidence for fetal viability:
Two identical twins will not have same:
Hasse rule is related to
Maceration is seen in death of?
A hair is found at a crime scene and you are asked to evaluate whether it is of human origin. Which of the following attributes indicates that the hair will be of human origin?
Which of the following is a characteristic feature of animal hair?
Practice by Chapter
Personal Identification Methods
Practice Questions
Anthropometry
Practice Questions
Dactylography (Fingerprinting)
Practice Questions
Dental Identification
Practice Questions
DNA Profiling
Practice Questions
Facial Reconstruction
Practice Questions
Superimposition Techniques
Practice Questions
Hair and Fiber Analysis
Practice Questions
Handwriting Analysis
Practice Questions
Identification of Remains
Practice Questions
Mass Disaster Victim Identification
Practice Questions
Age, Sex and Race Determination
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app