
Sudden and Unexpected Deaths — MCQs

An infant previously diagnosed with a large muscular VSD comes to the office with complaints from the mother of fatigue and poor feeding over the past month. You note the child has not gained weight since the previous visit 2 months ago. The child is apathetic, tachypneic, and has wheezes and crackles on lung auscultation. What is the most likely cardiac diagnosis based on this patient's presentation?
Autopsy finding after 24 hours in a case of death due to myocardial infarction is
What causes sudden decreased end tidal CO2 in GA?
A man who is chronic alcoholic will develop which type of cardiomyopathy?
Commonest cause of heart failure in infancy is:
What is defined as a negative autopsy?
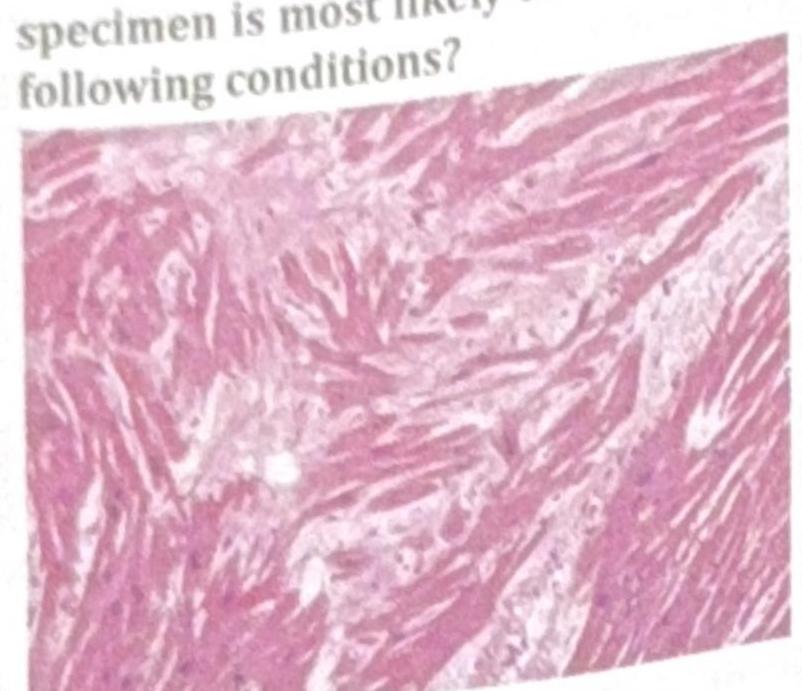
An athlete collapsed and expired while playing school basketball. Histology of the cardiac specimen is most likely to indicate which of the following conditions?
A healthy middle-aged man who became emotionally upset during an argument with his brother suddenly developed chest pain and collapsed. He was declared dead upon arrival at the hospital. What is the most likely diagnosis?
Which of the following statements about sudden infant death syndrome (SIDS) is false?
What does Casper's dictum indicate?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app