
Polysomnography — MCQs

Which of the following is a type of observational study that analyzes population-level data?
A 40-year-old man presents with daytime sleepiness and impaired concentration and memory. On examination his BMI is 41 kg/m2, BP is 160/100 mm Hg. His awake ABG analysis is given: PaO2=66 mm Hg, PaCO2=50 mm Hg, HCO3=28 mEq/L. What is the most likely diagnosis?
Berger waves (alpha waves) of EEG have a rhythm of how many Hz?
Most sensitive method of monitoring cardiovascular ischemia in the perioperative period is -
Which of the following is not a diagnostic criterion for SIRS?
A child presents with night blindness, delayed dark adaptation. Which investigation is to be done further to confirm the diagnosis?
In current obstetrics practice, what is the best test for monitoring sensitized Rh negative mother?
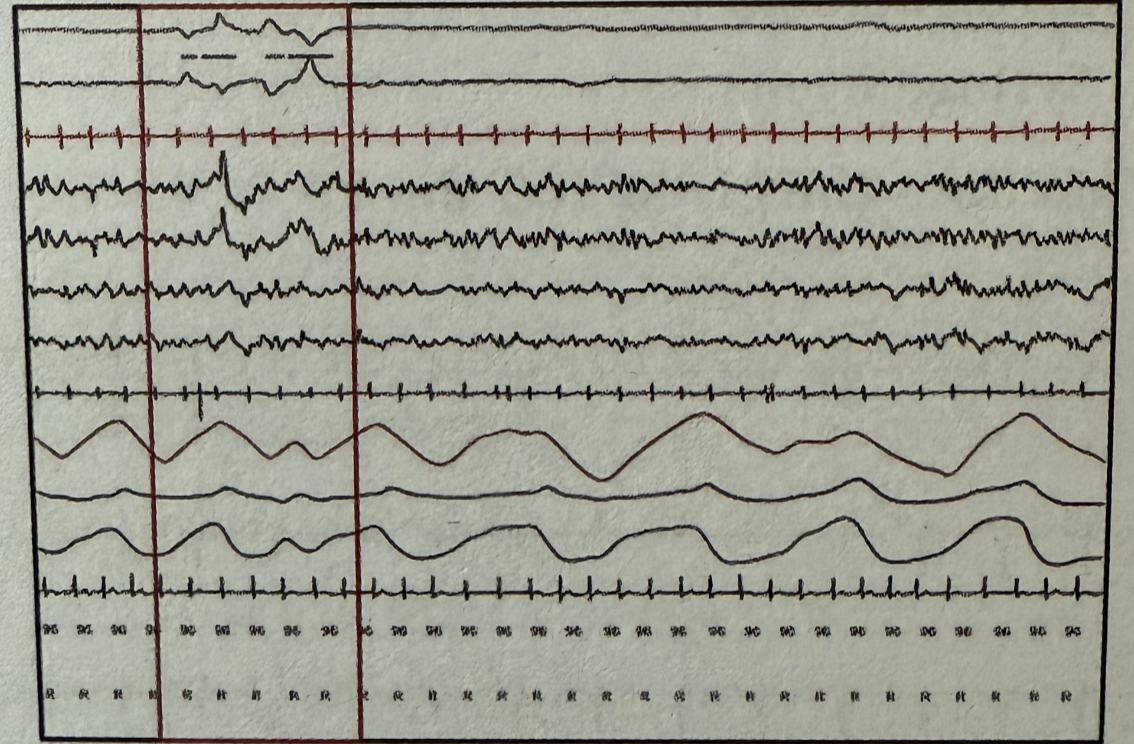
During polysomnography, which stage of sleep is represented by the marked areas when observing the following wave patterns? EOG (Electrooculography) EEG (Electroencephalography) EMG (Electromyography)
All of the following are correct about the image shown except:
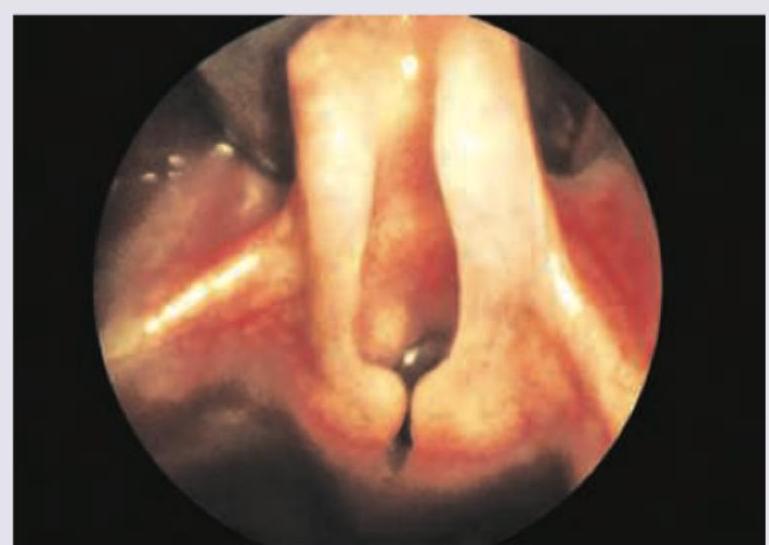
What is Muller's maneuver?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app