
Skull Base Chordomas and Chondrosarcomas — MCQs

What is the most common structural location within the bone for conventional chondrosarcoma?
All of the following statements about synovial sarcoma are true, except -
A 68-year-old man has many months history of progressive hearing loss, unsteady gait, tinnitus, and facial pain. An MRI scan reveals a tumor at the cerebellopontine angle. Which of the following cranial nerves is this tumor most likely to affect?
Which brain tumor is the most radiosensitive?
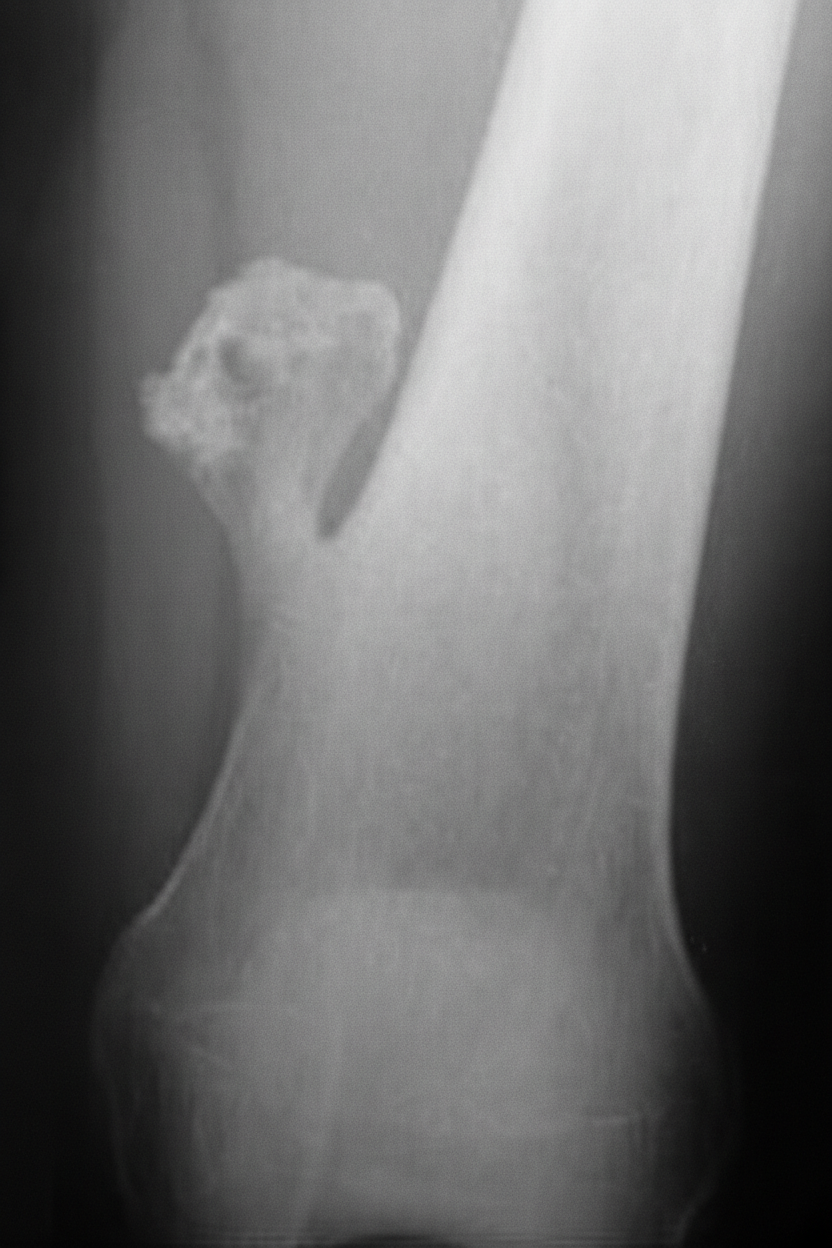
A 14 year old male presents with mushroom like tumor in the distal femur for past 2 years. Which of the following features suggest malignant transformation?
Which of the following is an epiphyseal tumor?
Nasopharyngeal chordoma arises from:-
Chordoma arises from:
A lady comes to OPD after fall from scooty. Her vitals are stable. She is having continuous, clear watery discharge from nose after 2 days. This is most likely a feature of?
FISCH classification is used for-
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app