
Endoscopic Skull Base Surgery — MCQs

Intrathecal fluorescein with endoscopic visualization is useful in diagnosis of?
A lady comes to OPD after fall from scooty. Her vitals are stable. She is having continuous, clear watery discharge from nose after 2 days. This is most likely a feature of?
Most difficult site to remove cholesteatoma from the sinus tympani is related to:
A nasal surgery was carried out with the incision shown in the image. What was the procedure likely carried out?

Which of the following is not a complication of maxillary sinus lavage and insufflation?
Which of the following is a common topical use of the medicine shown in the image?

Statement 1 - A 59-year-old patient presents with flaccid bullae. Histopathology shows a suprabasal acantholytic split. Statement 2 - The row of tombstones appearance is diagnostic of Pemphigus vulgaris.
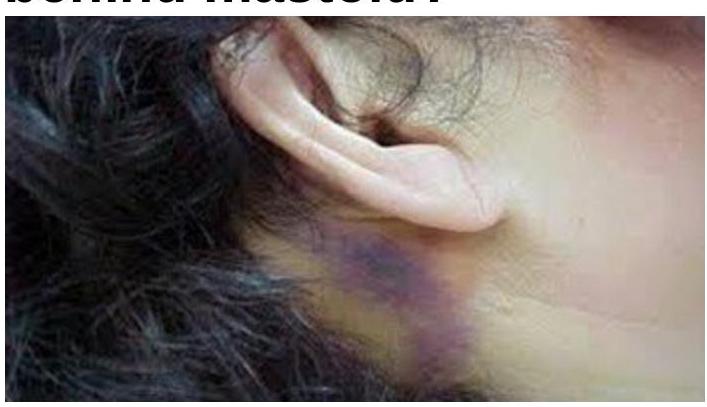
What does a bluish-purple discoloration behind the mastoid indicate?
FISCH classification is used for-
Dohlman surgery in Zenker's diverticulum is:-
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app