
Pediatric Hearing Loss — MCQs

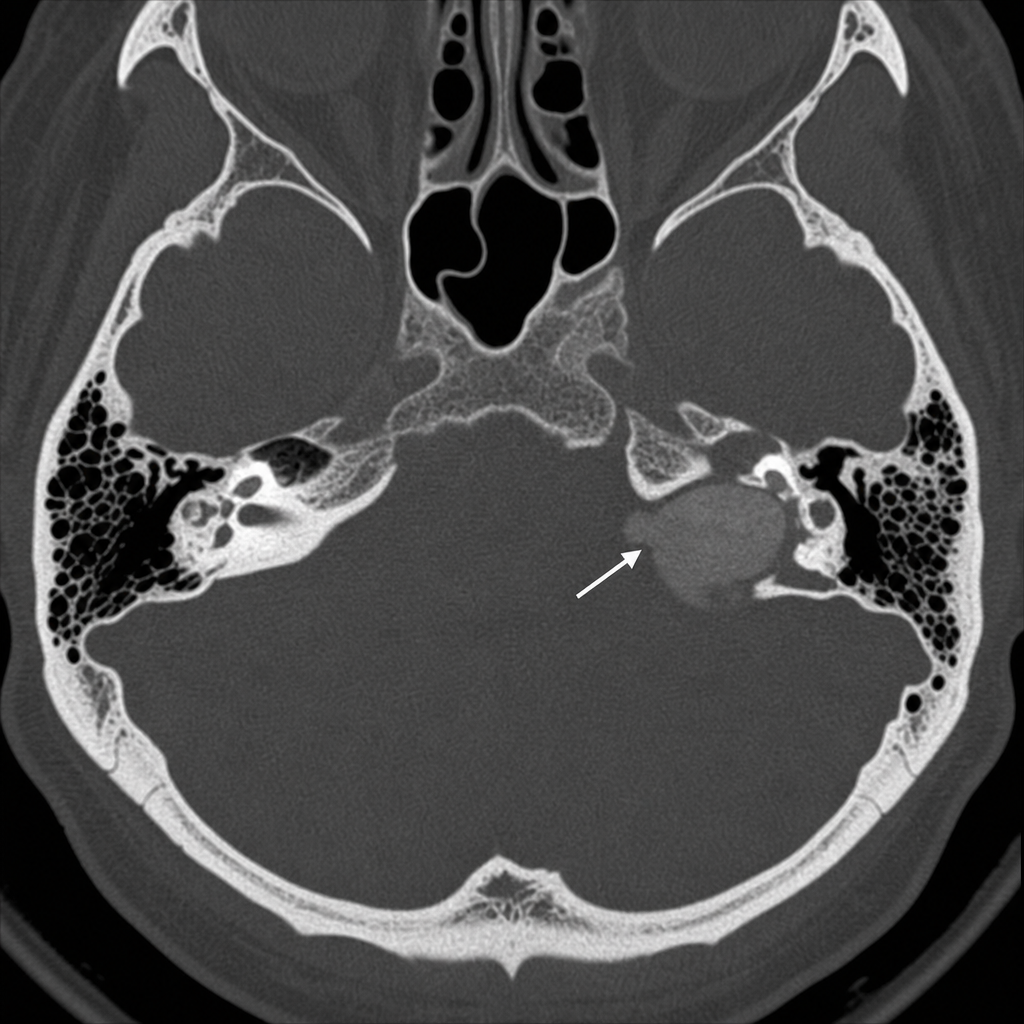
A patient presents with conductive hearing loss, pulsatile tinnitus and a positive Phelps sign. Using the CT scan provided, identify the condition.
Tests of SNHL are characterized by all EXCEPT
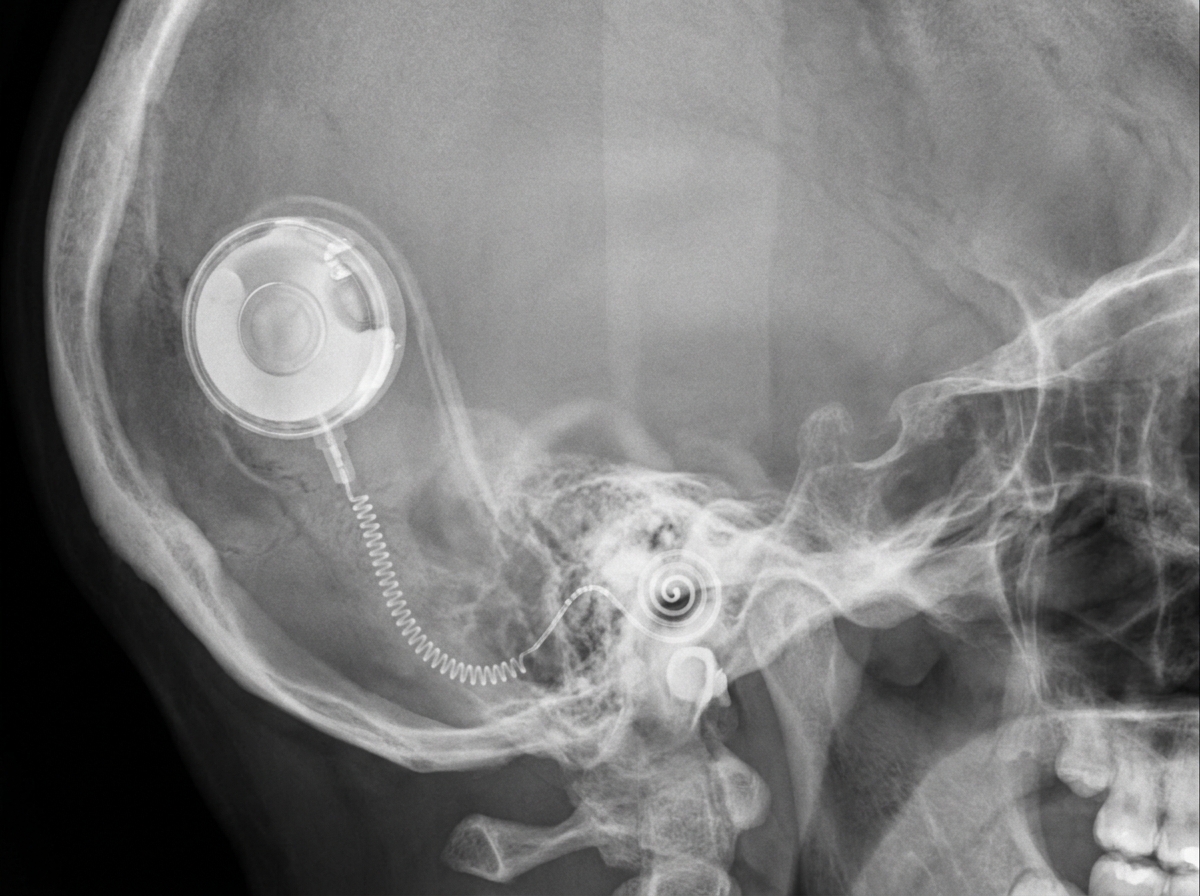
Which of the following would be the most appropriate treatment for rehabilitation of a patient, who has bilateral profound deafness following surgery for bilateral acoustic schwannoma?
Most common cause of syndromic deafness is:
Which is the investigation of choice in assessing hearing loss in neonates -
A child presents with recurrent ear infections and conductive hearing loss. What is the most likely diagnosis?
A first-grade teacher is concerned about a 6-year-old girl in her class who has not spoken a single word since school started. The little girl participates appropriately in the class activities and uses gestures, drawings, nods, and shakes her head to communicate. The parents report that the little girl talks only at home and only in the presence of her closest relatives. Which of the following is the most appropriate diagnosis?
Identify the device shown in the image below:

Which device is depicted below?
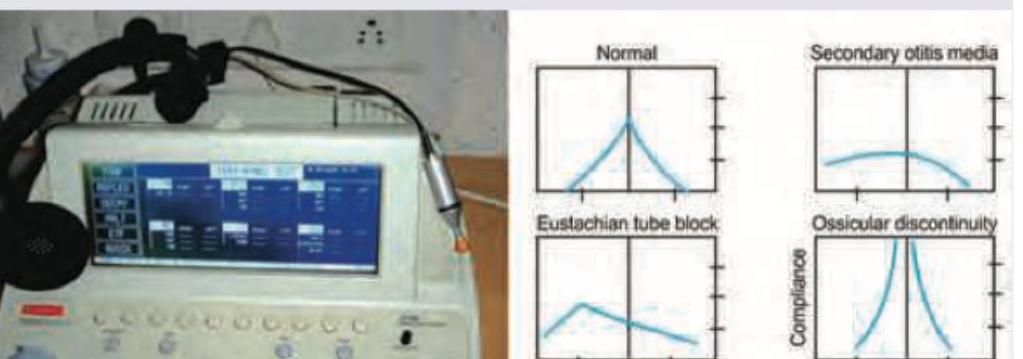
The following test is useful for diagnosis of all except:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app