
Otolaryngology Basics — MCQs

On this page
All of the following structures are adult-sized at birth EXCEPT?
Which of the following statements about Infraglottic carcinoma of the larynx is true?
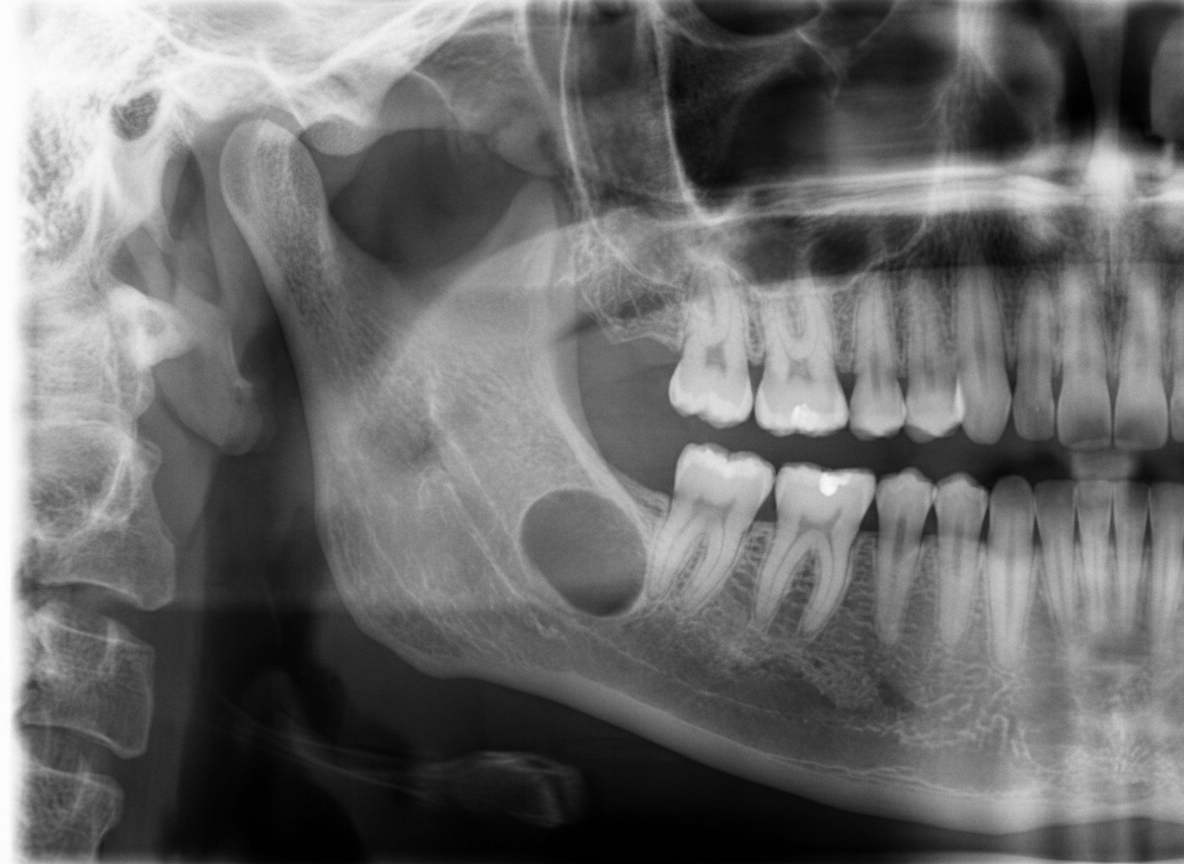
A 45-year-old male presented for a routine dental checkup. All teeth in the lower right quadrant were vital. A panoramic radiograph was taken. Which of the following can be the most probable diagnosis?
Phonation in esophageal speech in a patient who has undergone laryngectomy is produced by which structure?
What are the features of laryngeal carcinoma?
What is the recommended treatment for early vocal nodules?
Mouth opening is considered to be restricted when the distance is
Bryce's sign is seen in which of the following conditions?
What is the primary treatment for a mobile vocal cord tumor?
Eagle syndrome is also known as:
Practice by Chapter
Embryology of the Ear, Nose, and Throat
Practice Questions
Anatomy of the Ear
Practice Questions
Anatomy of the Nose and Paranasal Sinuses
Practice Questions
Anatomy of the Oral Cavity and Pharynx
Practice Questions
Anatomy of the Larynx
Practice Questions
Physiology of Hearing
Practice Questions
Physiology of Balance
Practice Questions
Physiology of Smell and Taste
Practice Questions
Physiology of Speech and Swallowing
Practice Questions
Clinical Examination in ENT
Practice Questions
Diagnostic Investigations in ENT
Practice Questions
Surgical Principles in Otolaryngology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app