
Otolaryngology Basics — MCQs

On this page
A 52-year-old woman presents with bilateral hearing loss noticed over the past 3 years. She denies tinnitus or vertigo. Otoscopic examination is normal bilaterally with intact, healthy tympanic membranes. Tympanometry shows bilateral type As (shallow) curves. The audiogram is shown in Image 1. She is medically fit for surgery but strongly wishes to avoid an operation at this time. Which of the following is the most appropriate next step in management?
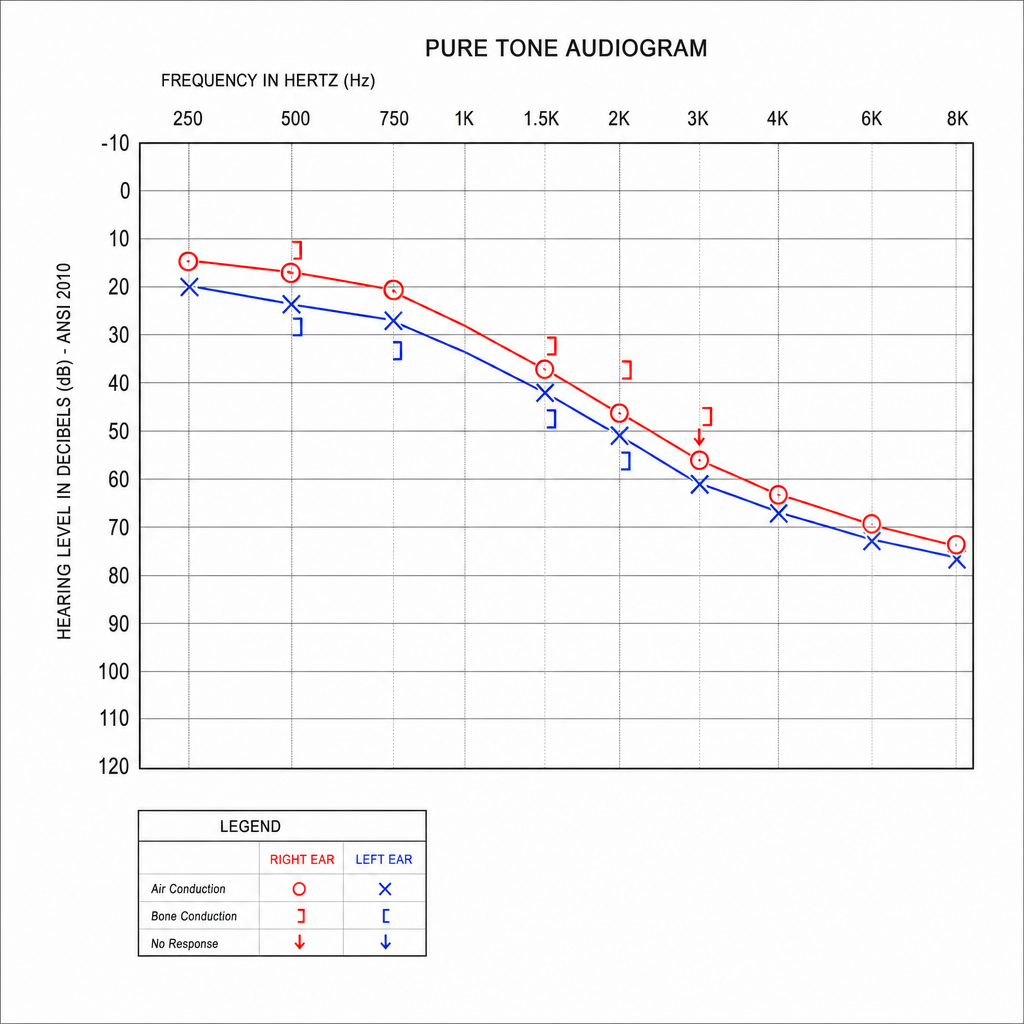
A 32-year-old woman presents with progressive bilateral hearing loss over 3 years, worse during pregnancy. She reports a family history of hearing impairment. Otoscopy reveals normal tympanic membranes bilaterally. Tympanometry shows As (shallow) curves. Her audiogram is shown (Image 1). Which of the following best explains the bone conduction dip seen on this audiogram?
Identify the instrument used in ENT surgery.

A patient with Pancoast's tumour develops loss of voice after radiation. What is the most likely cause?
Tracheostomy is indicated in all of the following conditions except:
The laryngeal saccules (water sacs) are present in which space?
Direct bronchoscopy can visualize all except?
All of the following structures are adult-sized at birth EXCEPT?
Hypothyroidism can cause all of the following symptoms except:
A Montgomery tube is used in which ENT procedure?
Practice by Chapter
Embryology of the Ear, Nose, and Throat
Practice Questions
Anatomy of the Ear
Practice Questions
Anatomy of the Nose and Paranasal Sinuses
Practice Questions
Anatomy of the Oral Cavity and Pharynx
Practice Questions
Anatomy of the Larynx
Practice Questions
Physiology of Hearing
Practice Questions
Physiology of Balance
Practice Questions
Physiology of Smell and Taste
Practice Questions
Physiology of Speech and Swallowing
Practice Questions
Clinical Examination in ENT
Practice Questions
Diagnostic Investigations in ENT
Practice Questions
Surgical Principles in Otolaryngology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app