
Vestibular Schwannoma Management — MCQs

The most common tumor of the cerebellopontine angle is -
All of the following are indications for Gamma Knife Radiosurgery EXCEPT
A 35-year-old man presents with progressive right-sided hearing loss, balance difficulties, and headaches. MRI reveals an enhancing mass in the cerebellopontine angle. Most likely diagnosis?
In a patient with acoustic neuroma all are seen except:
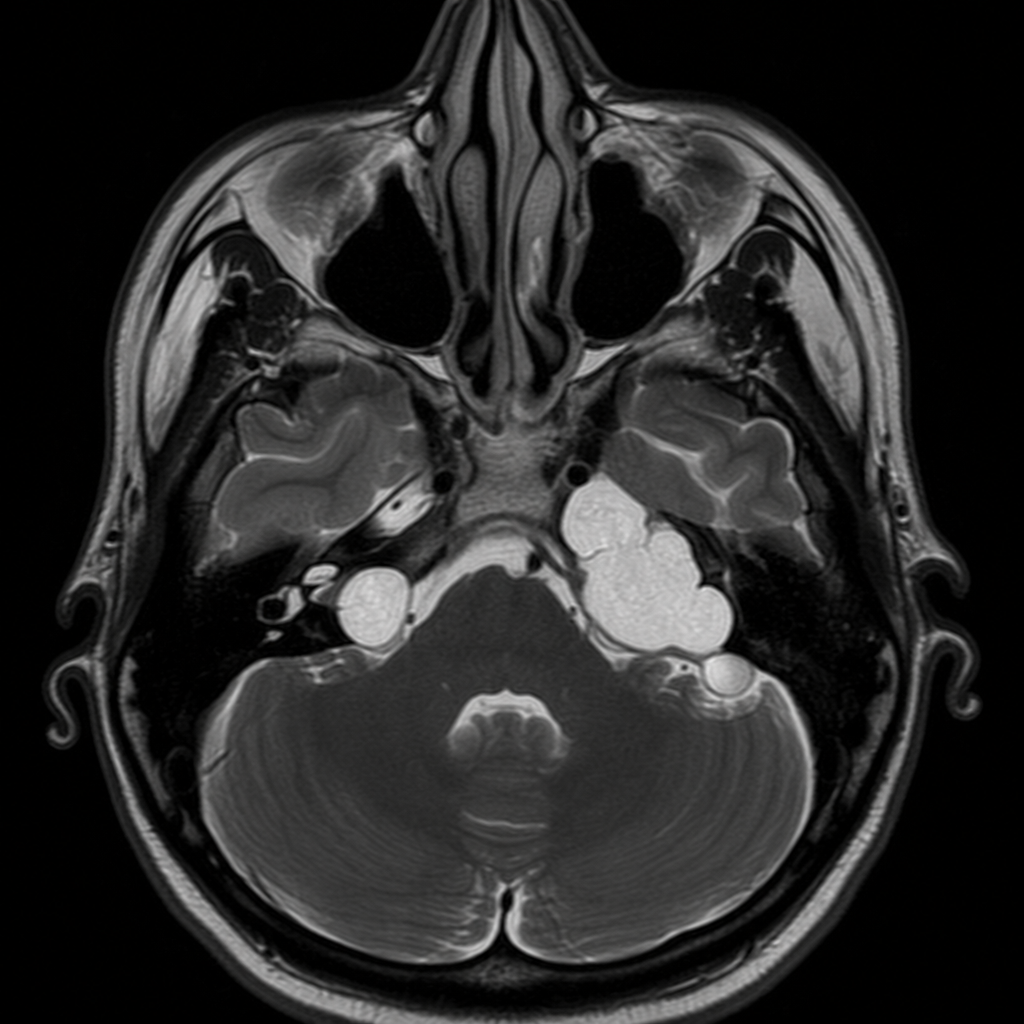
MRI done in a 28yrs old male suffering from Neurofibromatosis 2 showed ice cream cone appearance. On asking he further revealed that it began with ringing sensation in ears which progressed to balance problems and hearing loss. Which of the following is the most likely diagnosis -
Surgeries used in management of Meniere's disease are all Except
Most definitive treatment for large symptomatic acoustic neuroma is
True about acoustic neuroma:
All of the following cranial nerves are involved in Acoustic neuroma, except?
The most common brain tumour in an adult is
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app