
Neurotology — MCQs

On this page
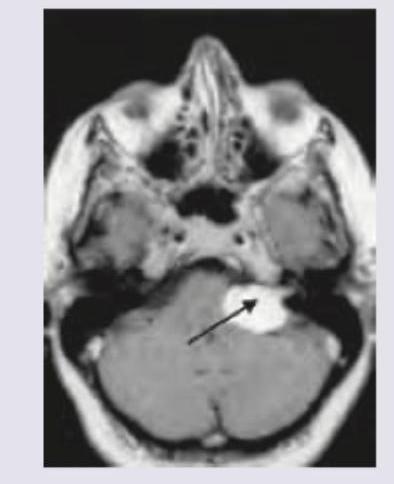
A 40-year-old female complains of progressive unilateral hearing loss and tinnitus. She also has developed numbness around posterior aspect of concha. MRI head was performed. What is the clinical diagnosis?
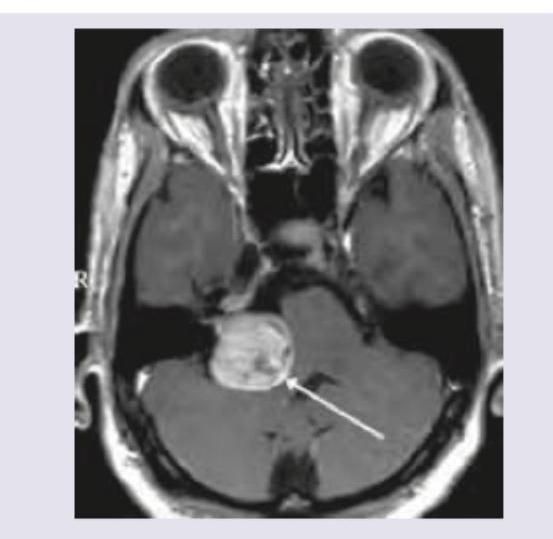
MRI Brain of a 40-year-old patient with progressive unilateral SNHL and tinnitus is shown below. Which is the most common extracanalicular nerve to be involved?
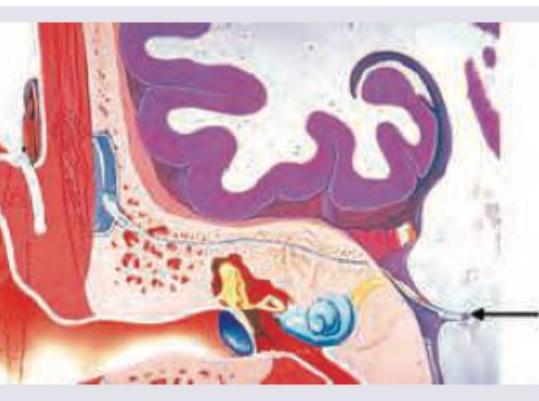
Which of the following hearing aid or implant is shown below?
True about acoustic neuroma:
Acoustic neuroma causes:
All of the following are true about glomus-jugulare tumor except:
The first clinical presentation of acoustic neuroma is characterized by ____________
Among the following non-auditory signs, which appears earliest in acoustic neuroma?
Which of the following would be the most appropriate treatment for rehabilitation of a patient, who has bilateral profound deafness following surgery for bilateral acoustic schwannoma?
A 35-year-old man presents with progressive right-sided hearing loss, balance difficulties, and headaches. MRI reveals an enhancing mass in the cerebellopontine angle. Most likely diagnosis?
Practice by Chapter
Vestibular System Anatomy and Physiology
Practice Questions
Vestibular Testing
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Ménière's Disease
Practice Questions
Vestibular Neuritis
Practice Questions
Labyrinthitis
Practice Questions
Acoustic Neuroma
Practice Questions
Other Cerebellopontine Angle Tumors
Practice Questions
Facial Nerve Disorders
Practice Questions
Skull Base Surgery
Practice Questions
Cochlear Implantation
Practice Questions
Vestibular Schwannoma Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app